|
W. J. Sidis Archive
Boris Sidis Archive Menu
I. RECURRENT PSYCHOMOTOR STATES. UNDER recurrent psychomotor states I include insistent ideas, imperative concepts, persistent or periodically appearing emotional states, irresistible impulses, as well as the psychomotor attacks of an apparently epileptic character which may be designated as “psychic epilepsy.” All those various states are found in many a symptom-complex of the insanities, but they are still more often met with the functional mental and nervous diseases,—in functional psychosis. In fact, in many forms of hysteria, in many types of neurasthenia, or of the more fashionable “psycho-asthenia,” recurrent psychomotor states constitute the main and often the only symptoms of the malady. The recurrent psychomotor states, with their great wealth of symptoms, appear almost mysterious in their onset and origin; they flash lightning-like on the patient’s mind, get possession of it, then disappear, only to reappear on some other favorable occasion. Others persist in consciousness, with but slight remissions, and keep the patient in a continuous agony. The patients are aware of the absurdity of the ideas and impulses, but they are powerless to resist them. They regard such onsets somewhat in the same way as the epileptics regard their attacks, which set on against will and consciousness, and which are not subject to control. I do not mean by it to indicate that all those psychic attacks are of an epileptic origin, but I only wish to point out the fact that there is some analogy between recurrent psychomotor states and epilepsy, inasmuch as both of them come on as sudden, uncontrollable attacks. It is true that in some cases we can drive the analogy more closely, because in some of the forms of recurrent psychomotor states we observe somewhat similar symptoms. We find the presence of a distinct aura, sensory in character, a sense of oppression, and sometimes a profound disturbance of consciousness during the attack, the patient occasionally being insensible to external stimuli. In some cases we even find a dazed state of consciousness, headache, and a condition of extreme fatigue after the attack is over. This resemblance, however, is but a superficial one. Recurrent psychomotor states differ widely from epilepsy. I have pointed this out in my previous works1 and shall show it in this paper by an analysis of cases selected from a number of others of the same type. Many writers are deceived by this superficial resemblance and regard such attacks as “larval epilepsy,” “as psychic equivalent of epilepsy.” Such a view is entirely unjustified by a close scientific analysis of the facts. The most that can be done is to draw an analogy between the attacks of insistent states and the attacks of epilepsy, but we must bear in mind that analogy is not a safe method, as one may find himself reasoning on the same lines with the Esquimaux, who regards glass as a kind of ice. Now it can be shown by rigid analysis of the cases of recurrent psychomotor states that they have nothing to do with epilepsy, although they may be associated with it, and that a study of the cases of recurrent psychomotor states reveals the fact of the presence of subconscious activities which become manifested as insistent ideas, uncontrollable emotions, irresistible impulses and various psychomotor states closely simulating epileptic attacks. It is from this standpoint that we may designate such simulating attacks as psychic epilepsy, not because they are psychic attacks, “equivalents” of real epilepsy, but they are pseudo-scientific attacks of a purely psychic origin,—they are manifestations of subconscious activities. One general characteristic of those psychomotor states is the fact of their recurrence with the same content of consciousness and with the same invariable motor reactions. The patient thinks, feels, wills and acts the same way. Subconscious dissociated states belong to the type of recurrent moment of consciousness, a type characteristic of the lower forms of animal life, which respond to external environment with the same adjustments, with the same psychomotor reactions. From this standpoint, we may regard the recurrent psychomotor states as a reversion to the lower forms of consciousness. The suddenness of the attack, the uniformity of the manifestations of the symptom-complex, the uncontrollable, overpowering effect on the patient’s personal consciousness are all due to the same underlying factor of dissociation of the patient’s subconsciousness. A disaggregated, subconscious life gives rise to recurrent psychomotor states,—to insistent ideas, imperative concepts, uncontrollable emotions, irresistible impulses, and to states of “psychic” epilepsy. There are many cases of insistent ideas and irresistible impulses which seem to contradict this law of uniformity and recurrence of psychomotor states which are seemingly of an evanescent character,—they are like stray comets coming out of the depths of space only to disappear again and never to recur. A close investigation will reveal the fact that the contradiction is but an apparent one. The various insistent ideas and impulses can in reality be referred to some few fundamental states persistently present in the subconscious and only appearing under different forms in the personal consciousness; they are like so many leaves and fruits of a single plant whose stem and roots are planted firmly in the subsoil of mental life. We may then say that all insistent mental states take their origin in a disaggregated subconsciousness and are periodic or recurrent in character, and as such may well be designated as recurrent psychomotor states.
II. CLASSIFICATION OF RECURRENT MENTAL STATES. We may possibly get better oriented in the vast domain of insistent mental states, if we make some provisional classification, however rough and unsatisfactory it may otherwise be. Now we may classify insistent mental states according to content and form. Classified according to content, we may divide insistent mental states into (1) conceptual or ideational, (2) ideo-motor, (3) sensory, (4) sensory-motor, (5) motor. According to form, they may be classified as, (1) desultory and (2) systematized. In the conceptual forms it is the general abstract idea that keeps on troubling the patient, such as the nature of God, the nature of Christ, or the nature of the Trinity and so on. The insistent ideas are here more or less of a metaphysical character. The patient does not feel satisfied with any answer. In many different ways the patient tries to raise difficulties to all kinds of possible answers. He tries to find loop-holes to escape from any solution, so as to have the question remain in full force. Were it not for the intense anxiety which is sometimes associated with such states, one would say that the patient delights in the mere process of questioning. He wants the problem, but refuses obstinately to accept the solution. In reality, however, it is not a matter of delight to the patient to persist in a state of problematic consciousness, so to say. Logical as the solution may appear to the patient, the problem is ever forced on the patient’s personal consciousness, for it is the work of dissociated states having their origin in a disaggregated subconsciousness. The insistent ideo-motor states refer to some act or motor activity which the patient has to reason out so as to know all the pros and cons, such as, for instance, whether it is right to play cards, or to read Sunday newspaper, or to visit theatre, or to travel on a Sabbath day. The patient gets lost in argumentations and discussions. He employs the most subtle casuistry, but he always meets with difficulties, never coming to any definite conclusions. Like the conceptualist, his mind is set entirely on the thought of the action which is never to become a reality. The patient’s will is thus paralyzed and he is in a state of doubt, indecision and hesitancy. The patient cannot accept any decision, however logical, as the same problem ever surges up in his mind with renewed vigor. What avails the patient’s reason against the blind dissociated forces, surging up from the depths of a disaggregated subconsciousness? The insistent sensory states comprise a wide domain of manifestations. All the insistent emotional states could be classed as sensory, since an emotion may be regarded as massive complex of sensory elements coming from various parts of the organism. Under this head we may include the functional states of depression and anxiety as well as the various phobias. Here also belong the various pains, headaches, hemicranias or migraines, when forming the main or central symptom of functional psychosis. The sensory symptoms of the hysterias, such as the anesthesias and hyperæsthesias, belong to the same category. All those states present the typical characteristics of the recurrent moment-consciousness. All of them can be referred to the dissociated experiences persisting in a disaggregated subconsciousness. What is manifested as the attack with the whole symptom-complex characteristic of it can be traced by a rigid analysis to an original experience which has occurred during the process of dissociation. The dissociated subconscious experience keeps on recurring as an attack. What goes under the name of hysterical stigmata can in reality be traced to dissociated subconscious experiences. During the attack the patient may preserve his personal subconsciousness fully or but partially. In such a case it appears as if two centers of consciousness are at work, one beside the other and one independent of the other. The patient may be aware of the new independent forces which are foreign to him, but which have apparently taken possession of him in spite of himself. The self seems to be torn in two, and consciousness is doubled. A new incipient parasitic personality is being formed in the recesses of the subconscious, a parasitic personality having a will of its own and no longer subject to the patient’s personal control. In other cases, again, the dissociated systems forming the parasitic personality may become fully manifested without the patient being aware of it. We have, then, two personalities in one organism working side by side, each apparently ignoring or not taking cognizance of the existence of the other. In other cases, again, the subconscious personality seems to take full possession of the principal focus of consciousness, the parasitic personality swamps the personal consciousness which sinks below the level of the active mental life and becomes submerged and no longer enters into active relations with the external environment. During such an attack the character of the person is changed and the memory is not bridged over as it is in the course of the normal associative activity, the functional recognitive elements are missing, consciousness may know of those experiences, but does not know them as its own. It is enough to outline here in a general way the possible lines of mental dissociation, as the discussion may carry one far into the domain of psychopathology. What we want to bring out is the fact that the phenomena of recurrent or insistent mental states range here though various stages of dissociation and that they can all by analysis be referred to a condition of a disaggregated subconsciousness. The sensory motor and purely motor are closely interrelated; sometimes the sensory and sometimes the motor symptom predominating in the total symptom-complex, when examined from a clinical standpoint. Here belong the various functional or hysterical visceral disturbances, hemiplegias, paraplegias, paralyses and contractures, also the functional tremors of psychic origin, all the states of “epilepsy” of the psychic type known under the name of “psychic epilepsy” which so closely simulate typical epileptic attacks. Finally, to the same category belong the various types of tics. The dissociated subconscious states may appear in consciousness in a disconnected, disseminated form,—they may appear as broken-up sentences, phrases and sounds, or of images having no relation with one another; they may come and go in great confusion, often producing a chaotic condition in the patient’s mind. The ideas keep on chasing one another, turning in circles without any rhyme and reason until the patient feels tired, exhausted and dazed by the kaleidoscopic whirl of the storm of ideas. Such insistent states may be designated as desultory. Quite often, however, the recurrent states are paranoidal in form. The ideas and feelings are well organized. The patient can give a clear interconnected account of his insistent states. In fact, the insistent states stand out in the patient’s mind so clear and definite that the patient can give a detailed analysis of all the minutiae of the condition. It seems as if his gaze is almost microscopically distinct, the least relation and outline are noticed. The insistent mental state seems as if fixed, so that the mental picture is strongly impressed on the patient’s consciousness and the vaguest detail cannot escape scrutiny. A wealth of associations are grouped around the central experience of the recurrent mental states, which form nuclei of highly organized groups of mental systems, arranged in an orderly array and logical relationship, forming an organic whole of a high degree of organization, the nature of which cannot be understood without a thorough exploration of the subconscious. Such recurrent mental states may be described as systematized. All those various manifestations can by close investigation into the patient’s subconscious life be traced to active dissociated systems, having their origin in a disaggregated subconsciousness. Of course, the reader must be warned not to regard my classification of the recurrent mental states as final. I made this classification to bring some order into that vast domain of mental life, so that we could make a brief review of the phenomena we deal with. The classification is simply a rough outline of the rough of the various phenomena that may have their origin in dissociated states of a disorganized, disaggregated subconsciousness. I should expect that the critical eye will detect in it a number of gaps, but the classification is offered as provisional one which may possibly serve for practical purposes.
III. MAIN TRAITS OF DISSOCIATED STATES. One point is worth while to bring out, and that is the fact of recurrence, so highly characteristic of the activity of dissociated subconscious states or moments-consciousness. The dissociated moment rises from the depths of the subconscious regions, oversteps the threshold of consciousness, manifests itself with an irresistible energy, throws the normal psychomotor reactions, for the time being, into a state of disorganization and then lapses from consciousness, only to be resurrected under conditions favorable to its activity. Such dissociated subconscious activities I describe under the term of recurrent moment consciousness. This characteristic of recurrence is of great importance in psychopathology, as it brings the subconscious activities under one perspective views, gives an insight into their nature and mode of manifestation; and from a biological standpoint brings them in line with the mode of action of the lower mental states, which respond to various stimuli of the external environment with the same amount and quality of sensori-motor reactions.3 The sense of reality is usually described, by writers on the subject, as not being affected. This is not the case. A close study of the facts shows that the insistent mental states come with an intensity of the sense of reality almost directly proportional to the insistence of the mental state which is truly delusional, or even hallucinatory, in character. This is especially true of the systematized recurrent states of the sensory type. The dissociated subconscious states refer to a past reality, now subconsciously real. In the ideational or conceptual forms the sense of reality appears to be weakened, because of the insistence of the ideational elements as contrasted with the sensori-motor elements. Another important and striking trait of the dissociated states is the violence, I would almost say vehemence, with which they become manifested; they reveal an amount of energy which similar states do not possess in the normal condition, when the personal consciousness is in active relation with the external environment. The energy displayed is more than the individual is capable of putting forth under ordinary conditions of life. The sudden mysterious onset of subconscious states, foreign to the whole character of the individual, as well as the sudden display of energies until now unsuspected in the person, make those states appear as mystical in the eyes of the populace and the superstitious. No wonder that the church has regarded subconscious activities as supernormal and miraculous and either ascribed them to divine powers or to satanic agencies and demonical possessions and obsessions. In our own time we have men devoting time and energy to the investigation of the supernormal nature of subconscious phenomena. In my previous works on the subject I have discussed the energy and violence of the eruption of subconscious forces as due to lack of inhibitions. This follows from the very nature of dissociation. Dissociated subconscious systems are being released from all relations with other systems and groups of mental elements, being let loose, so to say, from all associative bonds, will naturally display an amount of energy unusual for similar systems under the normal conditions of mental association. Still the phenomena of dissociation point to facts of a very important character. They point to an extremely important principle which I term “the principle of potential subconscious energy,” a principle which is of importance from a theoretical as well as from a practical therapeutic standpoint. I shall try to give a brief account of this principle of potential subconscious energy further on in this paper. Meanwhile, we should keep in mind two main characteristic traits of subconscious phenomena as manifested by dissociated states,—recurrence and latent energy. It may also be well to bring out another point of interest which holds true of the various types of insistent mental states,—they cannot be understood in the light of conditions under which they occur, or truer to say recur, since they bear no relation to their immediate environment, but to that under which the states have originally taken place. Unlike the mental states of the personal consciousness which are characterized by direct adjustments to the PRESENT conditions, the insistent subconscious states are adjustments to PAST conditions. May we not describe insistent or recurrent mental states as resurrected moments?
IV. HYPNOIDIZATION AND HYPNOIDAL STATES. In order to get at the dissociated subconscious states I have for many years employed a method which gives uniformly excellent results. I wish to attract the attention of the medical profession to this method of hypnoidization, as it is not only of theoretical importance for the purposes of psychopathological analysis, but is possibly of still greater value for practical therapeutic purposes. This is all the more requisite, as recently some medical men have confused method of hypnoidization with that of Breuer and Freud on the one hand and with Janet’s method of distraction on the other. The three methods are radically different and are based on widely different principles. The nature of the states obtained by the method of hypnoidization, as well as the character of the results, differ fundamentally from those of the other two methods. I shall return to this point further on in the study. An investigation of the nature of suggestibility carried out by me in a former work led me to formulate the following laws and conditions of normal as well as abnormal suggestibility. I do not think I shall be accused of plagiarism, if I take the liberty of quoting the table of normal and abnormal suggestibility from my “Psychology of Suggestion”:
It will be out of place in this study to give an account, however brief, of the experiments and discussion of the results arrived at; I can refer those are interested in the subject to the original work; for our present purpose it is enough to give here the principle laws formulated and the main results arrived at which will help to comprehend clearly the full significance of the method of hypnoidization. Now in the same work I come to the conclusion as the result of the investigation that “the nature of abnormal suggestibility is a disaggregation of consciousness, a slit, a scar, produced in the mind that may extend wider and deeper, ending at last in a total disjunction of the waking, guiding, controlling consciousness from the reflex consciousness. . . . Normal suggestibility is of like nature,—it is a cleft in the mind, only here the cleft is not so deep, not so lasting, as it is in the hypnosis or in the state of abnormal suggestibility; the split is here but momentary, evanescent, fleeting, disappearing at the very moment of its appearance.” We have also shown that the laws of normal and abnormal suggestibility may be stated as follows: “Normal suggestibility varies as indirect suggestion and inversely as direct suggestion. “Abnormal suggestibility varies as direct suggestion and inversely as indirect suggestion.” The general law of suggestibility is: “Suggestibility varies as the amount of disaggregation, and inversely as the unification of consciousness.” [Psychology of Suggestion, Chapter IX: Suggestibility and the Waking Consciousness.] Now it is on those general laws and nature of relation of the personal consciousness to the subconscious that I have based my method of hypnoidization. In order to reach the dissociated mental states we have to lay bare the subconscious, and this can be effected by the conditions requisite for the induction of normal or abnormal suggestibility, conditions which bring about a disaggregation of consciousness. In cases, therefore, where hypnosis is not practicable and the subconscious has to be reached, we can effect a disaggregation of consciousness and thus produce an allied subconscious state by putting the patient under the conditions of normal suggestibility: fixation of attention, distraction, monotony, limitation of the voluntary movements, limitation of the field of vision, inhibition and immediate execution. This is precisely what the method of hypnoidization consists in: “The patient is asked to close his eyes and keep as quiet as possible, without, however, making any special effort to put himself in such a state. He is then asked to attend to some stimulus such as reading or singing (or to the monotonous beats of a metronome). When the reading is over, the patient, with his eyes shut, is asked to repeat it and tell what comes into his mind during the reading, or during the repetition, or immediately after it. Sometimes the patient is simply asked to tell the nature of ideas and images that have entered his mind.” This should be carried out in a very quiet place, and the room, if possible, should be darkened so as not to disturb the patient and bring him out of the state in which he has been put. As modifications of the same method, the patient is asked to fixate his attention on some object while at the same time listening to the beats of a metronome; the patient’s eyes are then closed; he is to keep very quiet, while the metronome or some other monotonous stimulus is kept on going. After some time, when his respirations and pulse are found somewhat lowered, and he declares that he thinks of nothing in particular, he is asked to concentrate his attention on a subject closely relating to the symptoms of the malady or to the submerged subconscious states. The patient again may be asked to keep very quiet, to move or change position as little as a glass of water on a white background, with a light shining through the contents of the glass; a mechanism producing monotonous sounds is set going, and after a time, when the patient is observed to have become unusually quiet, he is asked to tell what he thinks in regard to a subject relating to his symptoms. He may be asked to write the stray ideas down, if speaking aloud disturbs the induced states favorable to the emergence of the dissociated mental states. In some cases it is sufficient to put the patient in a very quiet condition; have his eyes shut and command him to think hard of the particular dissociated states. This mostly succeeds in the case of patients who are also somnambulists. In short, the method of hypnoidization is not necessarily fixed, it admits of many modifications; it is highly pliable and can be adjusted to the type of case as well as adapted to the idiosyncrasies of the patient’s individuality. This method of hypnoidization has nothing in common with Freud’s method, nor with Janet’s method of distraction. Freud’s method is based on the course of normal associative activity, while the method of hypnoidization is based essentially on the process of dissociation by inducing a slight state of disaggregation of consciousness. From Janet’s method of distraction, that of hypnoidization differs fundamentally in that it is not at all based on distraction, but on the conditions of monotony, and sensori-motor limitations. In contrast to Janet’s method of distraction, hypnoidization may be characterized as the method of monotony.
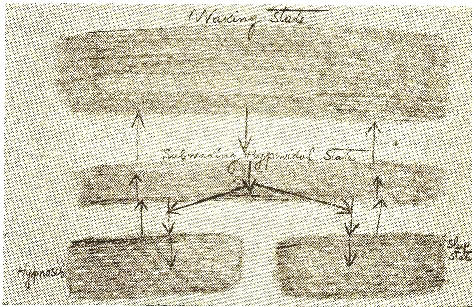
V. HYPNOIDAL STATES. What do we produce by the method of hypnoidization? We produce a peculiar state which, for lack of a better term, I designate as “hypnoidal.” What is the hypnoidal state? The hypnoidal state is essentially a borderland state. The subject is apparently awake and seems to be in full possession of all his powers, and still he is more closely in touch with the dissociated experiences than he is otherwise in the full waking state. Perhaps the subwaking state would possibly be an apt term for the hypnoidal condition. The subject seems to hover between the conscious and the subconscious, somewhat in the same way as in the half-drowsy condition we hover between wakefulness and sleep. The hypnoidal state is not a stable condition, it keeps on fluctuating from moment to moment; now falling more deeply into a subconscious condition in which outlived experiences are easily aroused, or again rising to the level of waking states. In such conditions the patient often tells you “something has come . . ., but it is gone.” The hypnoidal state has changed, it has become ligther, and the dissociated moments have become again submerged. There is a constant struggle going on in the hunting out of the stray dissociated systems. The state brought about by hypnoidization is essentially a transient, evanescent, mental disaggregation of the personal consciousness from the reflex subconsciousness. The hypnoidal state borders closely on light hypnosis; and still it is not exactly a hypnotic state and may be regarded as an intermediate state. In a series of experiments on the nature of sleep of lower animals as well of infants and adults, now being carried on by me at the physiological laboratory of Harvard Medical School and in my own laboratory, the facts tend to indicate that the hypnoidal state is intermediary between hypnosis and sleep on the one hand and the waking state on the other [see also An Experimental Study of Sleep ]. The relation may be represented by the following diagram:
The hypnoidal state may either lead to sleep or to hypnosis. The close relationship of the hypnoidal state and of hypnosis is sometimes forcibly brought to the attention of the experimenter. Some patients while in the hypnoidal state are observed to become unusually quiet, less talkative, become relaxed, and after a time a distinctly cataleptic condition of the extremities may be observed. The patient has apparently passed into hypnosis. In most of the cases the hypnosis is of very brief duration, while in a few cases the hypnosis may become lasting and deep. On the other hand, in many cases the subject falls into a sleeping state without as much as touching on hypnosis. The hypnoidal state is an intermediary state, intermediate between the waking state, and sleep hypnosis. Subwaking may possibly be an appropriate descriptive term of the character of the hypnoidal state. The subwaking hypnoidal state, like sleep and hypnosis, may be of various depth and duration; it may range from the fully waking consciousness and again may closely approach and even merge into sleep or hypnosis. The same patient may at various times reach different levels, and hence subconscious experiences which are inaccessible at one time may become revealed at some subsequent time, when the patient happens to go into a deeper level of the hypnoidal state. On account of the instability of the hypnoidal state and because of the continuous fluctuation and variation of the depth of its level, the subconscious dissociated experiences come up in bits and scraps and often may lack the sense of familiarity and recognition. The patient often loses the train of subconscious associations; there is a constant struggle to maintain this highly unstable hypnoidal state, and one has again and again to return to the same subconscious train started into activity for a brief interval of time. One must pick his way among streams of disturbing associations before the dissociated subconscious experiences can be synthesized into a whole, reproducing representatively the original experience that has given given rise to the whole train of symptoms. The hypnoidal state may sometimes reproduce the original experience which, at first struggling up in a broken, distorted form and finally becoming synthetized, gives rise to a full attack. The symptoms of the malady turn out to be portions, bits and chips of past experiences which have become dissociated, subconscious, giving rise to disaggregated subconsciousness. The method of hypnoidization and the hypnoidal states induced by it enable us to trace the history and etiology of the symptoms and also to effect a synthesis and a cure by means of methods which will be described further on. From the cursory discussion of the insistent psychomotor states, of the method of hypnoidization and hypnoidal states we can turn now to the cases.
VI. CASE OF RECURRENT STATES WITH SUBCONSCIOUS CHILD-LIFE. Mr. C., a young man of twenty-five, a college student of good standing, is very able, conscientious in his work, and is scrupulously moral in his daily life. Except for an aunt who has apparently died of tuberculosis, family history is negative. Parents are living and healthy, sisters and brothers are well. Both maternal and paternal branches of the family are of good healthy stock, with no neuropathic or psychopathic taint. The family is well to do, and the members are intelligent, educated and able, so that the patient’s childhood and early youth have passed amidst relatively healthy surroundings. As a child, the patient passed through children’s diseases, but did not suffer from any nervous troubles. As a boy he has been of robust health, taking great delight in physical exercises and pranks characteristic of boyhood. Although he is now of a rather serious, scientific turn of mind, devoting most of his time to mathematics, mechanics, and to the various branches of physical science, he has been in his childhood and boyhood very impressible and imaginative. He was a great lover of fairy tales, an omnivorous reader of all sorts of extravagant stories and of voluminous novels. Dreaming was his delight. Many a time he went off into a dark nook and kept on dreaming about princes and princesses; sailing in airships, ascending inaccessible mountains, scaling high peaks and then descending into mysterious caves and chasms. He lived in his imagination the world over and in all ages. Time and place were no barrier to him. He lived “the universe over and through eternity.” He lived with fairies, spirits and genii, who built for him enchanted palaces. He was “at the creation of the universe and saw the formation of the world.” Stories were to him histories, real histories in which he was the central figure, the real hero. When very young, he had auditory hallucinations,—“angels called him by name listened in dreams to the music of the spheres.” He ceased to have those hallucinations about the age of ten. On examination, patient was found well nourished. Reflexes not exaggerated; field of vision not limited; no sensory disturbances; no motor disturbances. Memory for disconnected impressions is good, while his recollection of past events and memory for present events are in excellent condition. No disturbances of recognition. Sense of localization is very good, so also is his sense of orientation. He is rather a good visualizer. A few times in his later years he experienced illusions of reversion of locality and also hallucinations of recognition of having seen the place before. Voluntary attention is in excellent condition. His conception of abstract ideas, his logical acuteness for points and distinctions, for comprehension of complicated trains of reasoning and for disputation by logical processes are truly remarkable. His sleep is very good and he has no bad dreams, though he is quite an active dreamer. The color field, on closure of eyes, is “brilliant,” and his hypnagogic and hypnapagogic4 hallucinations are often very rich and brilliant in color. Of late, the patient has been hard at work, studying for his examinations; he has been worrying over some family troubles as well as over his future career. He is somewhat nervous and restless, and occasionally a fit of irritability seems to take possession of him, an irritability which he sometimes has great difficulty to suppress. The patient complains of irritation of the bladder,—he cannot retain his urine for more than five minutes at a time and sometimes less than that. When he makes an effort to control his urgent desire to urinate, he is getting anxious, beings to feel hot, his eyes being to hurt and feel queer and bulging, and he has a very painful, distressing feeling of tension in his forehead, almost amounting to a severe headache. During that time he feels confused, his attention is wandering, his apprehension is for complicated trains of thoughts becomes defective, his desultory memory becomes extremely poor, he cannot repeat any series of disconnected syllables, while his logical memory for phrases and connected events becomes very vague. All those distressing symptoms are instantly relieved as soon as the pressing need for urination is satisfied. This insistent troublesome desire of urination disturbs the patient’s studies, interferes with his regular work, makes him undergo tortures in the lecture-room, or in church during services, or when visiting some friend. When, however, he gets greatly interested and absorbed in his work or in some conversation, the insistent distressing desire disappears for hours together. As soon as the interest lapses the insistent desire reappears. In addition to this insistent desire there is also present the insistent idea that along with the continuous outpour of the urine there is also an oozing out of his “vitality.” This fear of loss of vitality gives rise to an almost continuous examination of the urine to discover any abnormal changes. The color, the dribbling, the feel of the urine,—all are noticed and watched with a feeling of anxiety. The patient is conscious of the absurdity of the insistent idea, but he cannot help it. The idea gets the better of his reason. Occasionally, when he gets specially fatigued, an idea at which he feels extreme disgust enters his mind. When entering into a close conversation with a male person, the idea of homosexual relations gets possession of his mind. He does not have the least desire, in fact, he feels disgust at the very thought of it. He cannot account to himself for the reason of it, whether or no it is the horror of the idea which suggests it by association of contrast; he cannot understand it; the idea to his extreme disgust flashes on his mind; there is absolutely no desire accompanied with it, but deep disgust. The idea comes suddenly and as suddenly disappears. When the idea is gone, he afterward wonders how it could have possibly entered his mind at all. It appears to him so “idiotically stupid.” “Why should such a disgusting, stupid thought come to one’s mind?” The patient is also troubled by a form of jolie du doute. He is not sure that the addresses on his letters are correctly written; and no matter how many times he may read them over, he cannot feel assured that the addresses are correct. Some one else must read them and assure him that the letters are addressed correctly. In the absence of others he has devised the plan of copying the address from the envelope. This is somewhat more satisfactory, but then sometimes he is seized with the idea that may be the copying is wrong. Now and then he can help himself out by reading the address aloud. The seeing, reading aloud, the hearing of the words read and the feeling of pronouncing the words, along with the movements of copying—all those sensory stimuli seem to help intensify the sense of reality and increase the feeling of assurance in the “real correctness” of the address. When he has to write many letters sometimes a sudden fear gets possession of him that he had interchanged the letters and had put them into the wrong envelopes. He has then to tear open the envelopes and look the letters over and over again to assure himself that the letters have been put by him into the right envelopes. He becomes satisfied when assured by some one else. Before he drops the letters into the letter box he must repeatedly read over the addresses to be fully sure that he has the addresses all right. This condition is not a permanent one, as this whole trouble disappears for weeks and reappears when he is greatly worried or greatly fatigued. Similarly, in turning out the gas-jet he must needs try it over and over again, and is often forced to get up from bed to try again whether the gas is “really” shut off. He lights the gas, then puts it out, then tries to test the gas-jet with a lighted match to see whether the gas leaks and is “really” completely shut off. Similarly, in closing the door of his room, he must try the lock over and over again; he locks the door and then unlocks it again, then locks it once more, still he is not sure; he then must shake it violently so as to get the full assurance that the door has been actually and “really” locked. One is almost tempted to generalize that the sense of reality is weakened in the patient. But is it not strange that this weakness of the sense of reality should only be in relation to particular ideas and acts, while it is in excellent condition as far as all other ideas and acts are concerned? It is not the sense of reality then that is at fault,—it is the insistent idea. At one time he suffered from palpitation of the heart and he thought he had some heart trouble, for which he visited many physicians who kept on palpating, auscultating and percussing his heart, giving him all kinds of directions and precautions, putting him on a strict diet, regulating his exercises, prescribing bromides, digitalis and strychnine. But the more physicians regulated and prescribed, the more the refractory heart kept on thumping. Finally, losing patience, he gave up treatment and felt much better. Another trouble which has possession of him, though it is not very insistent, is the fear of getting consumption, or of being infected. Sometimes the fear becomes very troublesome, and it becomes a regular mysophobia, a délire du toucher; he may then keep on washing himself incessantly, rubbing his skin until it gets sore. Although the patient feels quite troubled, when the fear is on him, still it is not persistent; it seems to come in flashes, and he is quite free from it for long intervals of time. Still he has the feeling that the fear is there and it requires only special conditions to have it awakened. The mere sight of a supposed case of an infectious disease, or the contact with a tubercular patient, is sufficient to revive the state of mysophobia. There are again times when he feels as if his will is paralyzed. This condition comes on him at great intervals, when he happens to be very tired and he is in a state of abstraction and reverie. He feels as if he has no power of movement, he has hardly the strength to ask for a glass of water. When the water is brought to him he cannot reach out for it. He cannot account for this peculiar feeling that sweeps over him so suddenly. He knows well he is not paralyzed, and still he cannot move. It is an attack of abulia, it is his will that is paralyzed. After making one effort the spell is broken. Recently, an insistent idea has gotten hold of the patient’s mind, an idea which is very distressing to him and which makes him miserable. He thinks of tearing out his eyes and put them under some weight and have them crushed. If the patient sits in a chair he thinks of putting the eyes under the chair and have them crushed. If he goes in a car, he thinks of having his eyes crushed under the wheels of the car. He tells me that the insistent idea is sometimes so vivid and real that he can almost feel the cars passing over the eyes and that he can almost hear the eyeballs crush and crack. The patient fully realizes the absurdity of the idea, but it keeps on coming against his will. The idea comes in flashes, leaves for some time and then comes again when he expects it least. By means of the method of hypnoidization and hypnoidal states the following data were obtained: When a young child the patient lived with an old grandfather of his who suffered from bladder irritation with incontinence of urine, obliging the latter to go to the toilet-room almost every five minutes. He was very much attached to the poor old grandfather, whose sufferings evidently made a very deep impression on the child. The grandfather was also absent-minded and had to try to close the door or turn the key in the closet many times before he could fully be assured that the closet door was locked. The grandfather had also difficulty and hesitancy to handle the various things given him. When he asked for water, the glass given him was sometimes left on the tray for several minutes before he was reminded to take it. All this the child watched with great sympathy and distress. Being a highly impressionable, sensitive and imaginative child, can we wonder that his mind has been deeply impressed with what had taken place before him every moment of his young life? It was also in relation to his grandfather that he overheard people that “the vitality is oozing away.” In his childish mind he connected the oozing of vitality with the urination. All this was associated with anxiety and trepidation for the “oozing vitality,” and, though those sad experiences have all gone from the patient’s conscious memory, they have not, on that account, ceased their life existence,—they have simply lapsed from his personal consciousness, but only to become submerged into his consciousness these dissociated, disaggregated experiences of child-life kept on recurring as insistent psychomotor states with all the intensity of anguish of the original experiences. Instead, however, of the symptoms being associated with his grandfather, they have, by a very natural process of confluence and foreshortening, become grouped around the emotions which the patient has actually gone through at that time of his life, and have hence become associated with himself. The patient was living over again in his own subconscious life the life experiences of his deceased grandfather, experiencing all those various distressing symptoms for which the patient could consciously give no account. May we not in a certain sense say that the grandfather’s sufferings have been transmitted to the grandson? May we not say, be it in a figurative sense, that the grandfather’s life has become resurrected in the subconscious self of the grandson? The abulia manifested by the patient no doubt took its origin in what may be termed the subconscious “grandfather cycle” of experiences. Other experiences belonging to different cycles have also co-operated subconsciously and have helped to give rise to the state of will-defect. In one of the hypnoidal states it has come to light that, when the patient was very young, probably not more than six, he was taken to the bedside of a child of twelve who was stricken down with some form of paralysis. Once the experience struggled up in the hypnoidal state it stood out clear and distinct. The patient could in his mind’s eye see the courtyard, the house, the people and the paralytic child lying helpless in his little bed, a kind of crib. Even now when the subconscious experiences have become identified not as his own, he still feels a sinking sensation “in the pit of the stomach” and nearly feels the helplessness of the paralytic child. We can realize what a deep and lasting impression such an experience may have on the tender mind of an extremely sensitive and highly imaginative child. The great sensitivity and impressionability of the child can be gathered from another fact that also became revealed in one of the hypnoidal states. At about the same age of six or seven, the period to which the cycles of dissociated experiences belong and which have later on given rise to most of the distressing symptoms from which the patient has been suffering, when the child was in school, a man with a paralyzed right hand happened to come into the schoolroom. The child represented to himself vividly this same condition of paralysis in his own hand; he felt his hand and fingers growing powerless and his arm hanging limp by his side. Finally the feeling of helplessness and mental anguish became so intense, the paralysis so real that, overcome by his emotion, he fainted away. He was then sick for a few days. There is little doubt that such experiences have largely contributed to the patient’s abulic state in which his will to move his limbs and especially his hand is paralyzed. Now as to the homosexual ideas, what was the cause of ideas of sexual inversion, unaccompanied by any desire, foreign to the patient’s nature and associated with a feeling of almost “nauseating disgust”? In one of the hypnoidal states subconscious experiences emerged which, after a little tapping and close following of the course of warped train of consciousness, finally assumed the shape of the following connected account: When about the age of eight and a half he entered a private school in which there were also boys of the age of sixteen. Two of those boys gained his friendship and one day took him out for a walk into the woods. There they told him of a secret club they had formed and asked him to join it. The little boy was much pleased by an invitation to join a club of big boys. They then took him farther away into the woods into some lonely corner where they proceeded to enter into homosexual relations and urged him to imitate them, ending their urgings by forcible seizure. The little fellow got frightened and ran; the big boys gave chase, but they soon gave it up, as he hid himself in some thick bushes. He told his parents about it and was taken out of the school. This experience lapsed from his conscious memory, but remained firmly imprinted on his subconscious memory, giving rise to the apparently unaccountable homosexual ideas at which he felt so much disgust. The homosexual ideas were really foreign to his character and no wonder his whole nature felt revolting disgust toward them. There are other ideas, some of an insistent, some of a pleasing character, some of an apparently persisting æsthetic type, ideas and ideals, unaccountable on any other view, but on the theory of dissociated states and disaggregated subconsciousness. We cannot possibly describe here all of them, but we can bring a couple, typical of the rest. Why should the patient be pleased and even become sexually excited at the sight of a green petticoat? Why should the smell of heated iron, the sight and feel of starched clothes be so agreeable and even sexually exciting? Why should a prominent abdomen, large hips, long pendulous breasts, a few small black patches, interspersed with some little red pimples on the face have a sexual attraction and possess the significance of sexual stimulations? Why, again, should his ideal of feminine beauty be jet black, curly hair; large, black, lustrous eyes; a pale, somewhat dark skin; a pouting mouth; a low forehead and a slightly protruding chin? The method of hypnoidization and the hypnoidal states induced give an insight into those apparently unaccountable and whimsical mental states and reveal their origin in subconscious states of his early boyhood or childhood. Now in the hypnoidal states the image of a female figure emerged, a figure which the patient recognized as nurse of his whom he had up to his fifth year. She was a young woman of not more than thirty, of tall stature, with big hips and pendulous breasts, her face bearing the markings of small black plaster patches and red pimples. He sees her ironing some white goods while he tucks and pulls at her dress, at her green petticoat. She used to fondle him, kiss him, embrace him and press him to her breasts with which she often let him play. All those subconscious experiences of the patient’s childhood have helped to endow definite sensations and peculiar physical characteristics with an otherwise unaccountable attraction and sexual significance. Likes and dislikes, however trivial, especially if they belong to the fundamental instincts, are not accidental matters of chance, with no reason and meaning,—they can be traced, if one is sufficiently persistent with the hypnoidal state and the method of hypnoidization, to definite dissociated, subconscious activities. Similarly, in the case of the patient’s ideal of feminine beauty, the method of hypnoidization and the hypnoidal states brought out the underlying subconscious states. When the patient was of the age of seven he lived in the same house with his maternal aunt who had a little girl who was his companion in his plays and games, whom he worshiped and adored. It was that little cousin of his that had possessed all those physical characteristics,—black, curly hair; large, black, lustrous eyes; a low forehead; a pointing mouth; a pale, dark skin; a slightly protruding chin,—characteristics which have formed the ideal of his feminine beauty—gathered all the more latent force from the circumstance that the little girl fell a victim to an infectious disease, scarlet fever, and the little fellow stood at the deathbed of his little cousin. All those experiences may be regarded as belonging to the patient’s “sexual cycle” of subconscious life activity. We may turn now to other subconscious systems which may be designated as the “infectious cycle.” What is the origin of the patient’s mysophobia? Why and whence his fear of death and palpitation of the heart? As a very young child and at a very tender age he had a rather rich experience in witnessing death agonies. He was present at the deathbed of his great-grandmother just at the moment when she gave up her ghost in the arms of his grandfather; he also watched the death agonies of his aunt who died of tuberculosis. When at the age of seven and a half an epidemic of scarlet fever broke out in the house; his sister, his younger brother and the little girl, his cousin, fell victims to the contagious disease, and he was present at their deathbed. During the hypnoidal states an image of a figure suddenly appeared before the patient’s mind, held the hand over the heart, then fell with blood gushing from its mouth. The patient could not identify the figure, but he felt it was some real experience. It is quite probable that this related to some actual event of his very early childhood. The fear of infection and of death, as well as the palpitation of the heart consequent on such fears, were, by means of the method of hypnoidization and the hypnoidal states induced, traced, as have been the rest of the recurrent psychomotor states, to dissociated subconscious experiences. But why those insistent ideas about the eyes? For some time this could not be answered. One time, however, the patient happened to go into a deep hypnoidal condition, he fell into one of those intermediary states closely bordering on hypnosis. In this intermediary subconscious state new episodes from the patient’s child-life emerged. We may characterize this cycle of subconscious experience as “the great-grandmother episode.” An ancient great-grandmother of his lingered in the same house with the patient. While in his deep hypnoidal state the patient could clearly see the tall figure of his great-grandmother. She was greatly emaciated, skin and bone, and he stood in awe of her. Now this great-grandmother of his suffered from inflammation of the eyes. In his hypnoidal state the patient could recollect the many different liquids she used as washes for the eyes. She lived in a dark room and complained she could not see, the eyes pained her so much. And now a new experience emerged. Once the patient happened to get inflammation of the eyes. How he dreaded those great-grandmother bottles! And now he had to undergo the ordeal of having his eyes bathed by his great-grandmother’s various washes. He also remembers some horrible stories told of people who have pains in the eyes, how the eyes “swell and bulge and then crack and burst.” He also recollects stories of people with “glassy eyes,” who can take the eyes out and have them “crushed and cracked by passing objects.” We can well imagine what a deep and lasting thought subconscious, influence such gruesome tales may exert on the sensitive mind of a highly imaginative child. Thus by means of the method of hypnoidization and of the hypnoidal intermediary states the various threads of the complex web of insistent or recurrent psychomotor states with their concomitant symptoms have been traced to dissociated subconscious activities having their origin far back in the dim regions of the patient’s child-life. The dissociated subconscious experiences, like the moment consciousness of low types, kept on recurring with the same or similar mental content and psychomotor reactions, giving rise to apparently unaccountable, irrational, insistent ideas and emotions, deeply affecting the patient’s self-consciousness.
VII. CASE OF RECURRENT EPILEPTIFORM ATTACKS. M. L. is nineteen years of age, of a rather limited intelligence. He works as a shopboy amidst surroundings of poverty and leads a hard life, full of privations. He is undersized and underfed, and looks as if he has never had enough to eat. Born in New York, of parents belonging to the lowest social strata, he was treated with severity and even brutality. The patient has never been to any elementary school and could neither read nor write. His mathematical knowledge did not extend beyond hundreds; he could hardly accomplish a simple addition and subtraction and had no idea of the multiplication table. The names of the President and of a few Tammany politicians constitute all his knowledge of the history of the United States, the meaning of which is beyond his comprehension. Family history is negative, as his parents died when the patient was very young, and he was left without kith and kin, so that no data could possibly be obtained. Physical examination is negative. Field of vision is normal. There are no sensory disturbances. The process of perception is normal, and so also is recognition. Memory for past and present events is good. His power of reasoning is quite limited and the whole of his mental life is undeveloped, embryonic. His sleep is sound; dreams little, but wets his bed since his childhood. Digestion is excellent; he can digest anything in the way of eatable. He is of an easy-going, even gay disposition, a New York “street Arab.” The patient complains of “shaking spells.” The attack sets on with tremor of all the extremities and then spreads to the whole body. The tremor becomes general and the patient is seized by a convulsion of shivering and tremblings and chattering of teeth. Sometimes he falls down, shivering, trembling and shaking all over. The seizure seems to be epileptiform, only it lasts sometimes for more than three hours. The attack may come any time during the day, but is more frequent at night. During the attack the patient does not lose consciousness, he knows everything that is taking place around him, can feel everything pretty well; he only chatters violently with his teeth, trembles and shivers all over and is helpless to do anything. There is also a feeling of chilliness, as if he is possessed by an attack of “ague.” The seizure does not start with any numbness of the extremities, nor is there any anesthesia or parasthesia during the whole course of the attack. With the exception of the shivers and chills the patient claims he feels “all right.” Patient was put into a deep hypnoidal condition very close to the hypnotic state. There was some catalepsy of a very transient character, but no suggestibility of the hypnotic type. Now in this hypnoidal state it came to light that the patient “many years ago” was forced to sleep in a dark, damp cellar where it was bitter cold. The few nights passed in that cold cellar he had to leave his bed, and shaking and trembling and shivering and chattering with cold he had to go to urinate, fearing to wet his bed, in expectation of a severe punishment. The patient, while in that intermediary, subwaking, hypnoidal state, was told to think of that dark, damp, cold cellar. Suddenly the attack set on,—the patient began to shake and shiver and tremble all over, chattering with his teeth, as if suffering from great cold. The attack was thus reproduced in the hypnoidal state. “This is the way I have them,” he said. During this attack no numbness, no sensory disturbances, were present. The patient was quieted, and after a little while the attack of shivering and cold disappeared. Now the room in which the patient was put into the hypnoidal state was very dark, and accidentally the remark was dropped that the room was too dark to see anything; immediately the attack reappeared in all its violence. It was found later that it was sufficient to mention the words “dark, damp and cold” to bring on an attack even in the fully waking state. We could thus reproduce the attacks at will,—those magic words had the power to release the pent-up subconscious forces and throw the patient into convulsions of shakings and shiverings, with feeling of cold and chattering of the teeth. Thus the apparent epileptiform seizures, the insistent psychomotor states of seemingly unaccountable origin, were traced to dissociated systems of a disaggregated subconscious.
VIII. RECURRENT STATES WITH TROPHIC DISTURBANCES AND EPILEPTIC ATTACKS Mrs. L., sixty years of age; married. Family history is good. Parents died of old age; brother died of apoplexy. Patient had one daughter who died some fifteen years ago. The patient complains of sensitiveness of the stomach, of kidney trouble and of nervousness. During the attacks of nervousness she is restless, sleepless and is underground “death agonies.” The suffering is so intense that, in spite of her religious scruples, the thought of suicide forces itself on her mind. She has an insistent fear of getting insane; the fear is so intense that she paces the floor night after night, like an animal in a cage. She is unable to eat and hardly drinks anything when the attack is on. If she attempts to eat, she rejects it immediately, as the stomach seems to be then extremely sensitive, so that she cannot retain anything. “While my brain is perfectly clear to take up any intellectual pursuit, if I attempt, for instance, to purchase anything in the way of apparel, my brain gets on fire and I walk the floor in a frenzy of excitement, not having the least idea as to the choice I should make. I am not able to sleep or eat, and what little food I eat does not digest. Although so disabled in judgment as to myself, my friends often come to me to aid them in their decisions in matters of apparel, because they value my judgment, which is perfectly cool, when I am deciding for them.” Though the oculists do not find anything special the matter with her eyes, she complains of weakness and occasionally of complete darkness settling on the eyes, at first in the form of a mist and then, becoming denser, ends in total darkness, a form of functional amblyopia. She also complains of severe headaches,—the head feels at first dizzy, sore, painful, throbbing, and very hot, as if it were on fire. Patient also complains of trophic disturbances, of a dry skin, of swellings and rashes on the body. For years she has been suffering from those trophic disturbances which she terms “erysipelas.” When the attack sets on, the patient becomes greatly depressed,—the hands and feet are cold; the bowels are constipated; there is irritation of the bladder, tinnitus aurium is present; there is a feeling of pressure in the head with dreams of a distressing character; then the headache grows in severity and becomes throbbing. After a time trophic disturbances appear, such as rashes in the form of “pimples and swellings,” with edema of the legs, of hands and eyes. Now and then the patient has seizures of coughing spells and has insistent fears of some impending lung troubles. Occasionally she has epileptiform attacks with slight tonic and clonic convulsions, accompanied with unconsciousness or semi-conscious. Some years ago she used to have “attacks of helplessness” and even of complete paralysis. She also suffered from tingling sensations in the extremities, “numbness all over,” becoming fully anesthetic over the whole surface of the body. An examination of the patient shows her to be greatly emaciated; poorly nourished; skin is dry and crackling. There are a few macules and papules, a few wheals and the remnants of dried-up vesicles and blebs. Near the margin of the mucous membranes some fissures and excoriations are found in various stages of healing and crusting. The tongue is coated, furred and there is a heavy smell from the mouth. The lungs are in good condition. The heart-beat is irregular, aortic second sound is slightly accentuated. Patellar reflexes are greatly exaggerated. The eyes do not accommodate well,—the left eye is somewhat defective in convergence during the act of accommodation. Pupillary reaction is rather sluggish. The tympanic membrane of the left ear is slightly thickened and hearing is defective on the left side. She also suffers occasionally from noises, “buzzing in the head” and dizziness. Motor activities and sensitiveness to all forms of sensory stimulations are in good condition. No edema could be found, except a slight puffy condition below the eyes. Several examinations of the urine showed the latter free from any trace of albumin. Patient can see well, but she gets easily fatigued when reading or sewing,—a darkness then comes over her and everything seems to be enveloped in a mist which is getting heavier and thicker. Field of vision is fully normal. No reversion of the color field is present. Memory for present and past events is excellent. Attention is very good, but she cannot keep up her concentration of attention for any length of time; she then begins to complain of fatigues and sometimes gets an attack of severe headache, with all the symptoms associated with it. Intellectual powers are well preserved and, in fact, are quite vigorous. Patient is well educated, writes well and has a deep interest in philosophical, especially in theological, problems. Hypnagogic and hypnapagogic hallucinations are well developed; field of vision on closure of the eyes is very rich in colors. Sleep is greatly disturbed, she suffers from insomnia, and when she falls asleep she has quite elaborate dreams, often of a distressing character. Once she had a visual hallucination of her daughter, and another time she had the peculiar hallucination of the reality of the presence of her daughter, who did not appear to the “bodily senses,” but to the “inner mental vision,” a form of pseudo-hallucination. She has a yearning after something, she does not know what, and is in constant fear of losing her mind. The fear of insanity is occasionally so intense that she suffers agony. Her general mood or affective state is one of great depression and misery. The hypnoidal states revealed the following data: When at the age of five, the patient happened to see an insane woman in a maniacal condition. The image of that woman never left the patient’s thought, conscious or subconscious, so deeply was her mind impressed with that event. She was greatly frightened and the thought kept recurring: “Do little girls get insane?” Since that time she became possessed by the fear of insanity. In her ardent imagination she actually felt she was getting insane. When asked about her dreams, the patient was unable to tell anything, but in one of the deeper hypnoidal states she remembered that she used to dream about that insane woman standing near her bed, bending over her and even touching her. Many times she was in such an agony of fear that she wanted to cry out, but was unable to do it. When she woke up, she cried in great terror. When the patient gave birth to her child, she was afraid the child would get insane; many a time she even had the feeling as if the child was insane. Thus the fear of insanity is traced to an experience of early childhood, an experience which, having become subconscious, is manifesting itself persistently in the patient’s consciousness. The patient’s parents were very religious, and the child was brought up not only in the fear of God, but also in the fear of hell and the devil. Being sensitive and imaginative, the devils of the gospel were to her stern realities. She had a firm belief in “diabolical possessions” and “unclean spirits”; the legend of Jesus exorcising in the country of the Gadarenes unclean spirits, whose name is Legion, was to her a tangible reality. She was brought up on brimstone and pitch, with everlasting fire of the “bottomless pit” for sinners and unbelievers. In the hypnoidal state she clearly remembered the preacher who used every Sunday to give her the horrors by his picturesque descriptions of the tortures of the “bottomless pit.” She was in anguish over the unsolved question: “Do little sinner-girls go to hell?” This fear of hell made the little girl feel depressed and miserable and had poisoned many a cheerful moment in her life. What a lasting effect and what a melancholy gloom this fear of ghosts and of unclean spirits of the bottomless pit produced in this young life may be judged from the following facts: When the patient was about eleven years old, a young girl, a friend of hers, having noticed the patient’s fear of ghosts, played on her one of those silly, practical jokes, the effects of which on sensitive natures are often disastrous and lasting. The girl disguised herself as a ghost in a white sheet and appeared to the patient who was just on the point of falling asleep. The child shrieked in terror and fainted. Since that time the patient suffered from nightmares and was mortally afraid to sleep alone; she passed many a night in a state of excitement, frenzied with fear of apparitions and ghosts. When about the age of seventeen, she apparently freed herself from the belief in ghosts and unclean powers, but the fear acquired in her childhood did not lapse, it persisted subconsciously and manifested itself in the form of uncontrollable fears. Unless specially treated, fears acquired in childhood last through life.5 She was afraid to remain alone in a room especially in the evening. Thus, once when she had to go upstairs alone to pack her trunks, a gauzy garment called forth the experience of her ghost-fright,—she had the illusion of seeing a ghost and she fell fainting to the floor. “An old soldier whom I asked what his greatest fears had been, answered me thus: ‘I have only had one, but it pursues me still. I am nearly seventy years old, I have looked death in the face I do not know how many times; I have never lost heart in any danger, but when I pass a little old church in the shades of the forest, or a deserted chapel in the mountains, I always remember a neglected oratory in my native village, and I shiver and look around, as though seeking the corpse of a murdered man which I once saw carried into it when a child, and with which an old servant wanted to shut me up to make me good.’ Here, too, subconscious experiences have persisted throughout lifetime.” When about the age of eighteen, she began to teach mathematics in a school and worked very hard. Being ambitious to advance, she studied assiduously after she was through with her school duties; she worked hard and worried much over her prospects of advancement. It was from that period that her headaches date as well as her first attack of nervous prostration. When she got married, the duties of housewife and of social relations made life still more strenuous. Motherhood served only to increase the nervous strain, all the more so as her child was constantly ailing up to the age five. After years of devotion and of methyl self-sacrifice she succeeded in binging up her daughter, who became the very soul of the patient’s being. What a fearful blow it must have been to this frail woman when her only daughter, in the full bloom of her young womanhood, at the age of twenty, began to ail, to sink in health, and was declared an incurable case of tuberculosis. Day and night did the unfortunate mother watch in anguish over her only child. She actually lived through the distressing cough, the gastric and trophic disturbances, the loss of appetite, the nausea, the inability to retain food, the weakness, the helplessness and the complete prostration of her daughter who did her best to cheer her poor suffering mother who, with an aching heart, eyes blinded with tears and with a mind distracted by anguish and anxiety, felt her head in a whirl; choking sensations, darkness, fainting spells began to seize on her, spells of darkness against which she struggled in throes of convulsions. In one of the hypnoidal states I happened to press on the throat, accidentally producing choking sensations, when the patient began to feel faint and, losing consciousness, became convulsed with epileptiform tonic and clonic contractions. The state of unconsciousness, of semiconsciousness or of “Dämmerzustände,” lasted about twenty-five seconds, the patient coming back with a deep sigh and with no memory of what had taken place during the attack. I was thus enabled to reproduce at will the original attacks. The patient told me that with all her “faith in the Lord” she rebelled against “Providence.” “I have blasphemed the Lord,—He is worse than a loving mother.” The daughter passed away in the arms of the mother, who from that time on had been living through the diseases of her child with all the symptoms of trophic disturbances and death agony, but much more complicated and intensified by the agony which she herself had then undergone. Dress, receptions, visits became painful to her, because of the daughter with whom all those enjoyments have been associated. The whole life experience of that period of anguish has left but a vague trace, has apparently lapsed from the patient’s consciousness, but has really persisted in her subconsciousness and has been forcing itself with all the more vehemence on the patient’s personal self. All those symptoms, however, entirely disappeared during the treatment. Thus the whole symptom-complex of the disease could by means of the hypnoidal states be traced to dissociated, submerged subconscious experiences recurring in the form of attacks of insistent mental states or of current psychomotor states.
IX. PERSISTENT FEARS WITH ATTACKS OF HEMICRANIA. Mr. D., a young man of twenty-five. Born in Poland. Family history could not be obtained, but as far as it could be ascertained the parents as well as the brothers and sisters are all well. An examination of the patient reveals nothing abnormal as far as the physical and mental functions are concerned. Patellar reflex is but slightly exaggerated. There are no sensory, no motor disturbances. Hypnagogic and hypnapagogic hallucinations are rich and varied. The emotional side is fairly well endowed. He is a level-headed fellow, but unusually timid. The patient complains of severe headaches, often setting on gradually and preceded by a feeling of indisposition, depression, vertigo and distress. During the attack there is hyperæsthesia to touch, pressure, temperature and to visual and auditory stimulations; the body feels cold and ataxic, as if paralyzed. The patient shivers and looks very pale. The periphery of the extremities is bloodless, cold; the face is very pale, the lips are cyanotic, while the head throbs violently. The cold experienced is so intense that the patient has to wrap himself in many blankets, as if suffering from an onset of malaria. Fears have a strong possession of the patient’s mind. He seems to suffer from claustrophobia,—he is afraid to remain in a closed place at daytime and especially at night, but he is not afraid to be on the street, even when it is very dark. When he has to remain alone at night, he is in agony of fear and cannot go to sleep. Every passer-by is regarded as a robber or murderer, and he quakes at the least noise. When walking in the house in the dark, he has the feeling as if some one is after him, and occasionally even experiences the hallucination of some one tugging at his coat. He is mortally afraid of the dead and shuns a funeral, not on account of superstition; in fact, he is ashamed of it, but on account of some insistent fear that takes possession of him in spite of all his efforts to control it. He has a feeling of weakness almost of prostration, not unmingled with some unaccountable fear, when he as to visit a cemetery, even if it be broad daylight and in the company of many people. Any strange object he suddenly comes across in the dark will give the patient the shivers. This fear is very intense, when he happens to notice in the dark a moving object. Besides the claustrophobia, the patient has also a fear of dogs, a kind of kynophobia, so to say, if we may be permitted to use such a term. The fear is irresistible and is almost as involuntary as a reflex. The patient’s sleep is restless and disturbed by many distressing dreams and nightmares. He dreams of fires, of great conflagrations in which he is in great danger and cannot find his way out of buildings enveloped in sheets of flame and dense smoke. He dreams of being captured by robbers and is in danger of being killed or even of being skinned alive. Occasionally he dreams of his parents captured and assaulted by brutal, terrible looking men. Thus is one of his recent dreams he saw his father seized by soldiers, imprisoned and condemned to be hanged. The patient often moans in his sleep, cries and wakes up with tears streaming down his cheeks. The anguish experienced in his dreams is intense. So vivid is the dream-consciousness that the patient cannot get over his anxiety for hours and he is sometimes affected by it throughout the next day. Occasionally the patient dreams that wild animals, such as wild dogs, attack him and he wakes up in great fright. So intense is the dream hallucination that the fear persists long after he is awake, and he feels as if he has actually gone through a real experience. An investigation by means of the hypnoidal or intermediate states brought forth out of the patient’s subconscious life the following experiences: When a child of three, the patient lived with his family a small village near a large forest infested with wolves. In one of the intermediary states a faint memory, rather to say a vision, struggled up,—a vision of wolves and dogs. Some one cried out: “Run, wolves are coming!” Crazed with fear, he ran into the hut and fell fainting to the floor. It turned out to be dogs instead of a pack of wolves. It is that fright in early childhood which has persisted in the subconscious and, having become associated with subsequent experiences of attacks of dogs, has found expression in the patient’s consciousness as an almost instinctive fear of dogs. When about the age of four, the patient went through another experience which left an indelible impression on his subconsciousness. One winter night a fire broke out in the house and the little boy had to be taken out, shivering with fright and cold, into the open air of a frosty night. When about the age of eight, the patient, then living in a small provincial town, experienced another similar shock. A great conflagration broke out in the street where the patient lived. The fire, carried by the wind, spread rapidly, so that his house was enveloped in flames and smoke. The patient was so terrified that he was almost in a trance. He seized a saltcellar, rescuing it from the flames, and fled. For six hours his parents lost all trace of him. He himself could not remember where he had been. It was afterwards found that he kept on running through the streets, crying: “Fire, fire!” He was found by relative of his took away from him the saltcellar and quiet his agitation. Subconsciously the patient kept on living through those very experiences in his dreams. The experiences lapsed from his consciousness, but persisted in his subconsciousness and found expression in his dream hallucinations, which appeared as real experiences to his subconsciousness. The content of the dreams is varied, largely depending on the sensory content of the total moment-consciousness, but it refers to the same dissociated systems of the patient’s child-life. But why was the patient in such abject terror of dead people? This found its answer in the experiences and training of his early life and especially in a peculiar incident experienced by the patient in his childhood. When a very young child, the patient heard all kinds of ghost stories and tales of wandering lost souls and of spirits of dead people hovering bout the churchyard and burial grounds; he heard gruesome stories ghouls and evil spirits inhabiting deserted places, dwelling in the graves of sinners and the wicked. He listened to stories of haunted houses and of apparitions stalking about in the dark, coming to visit the living in some lonely deserted places, especially in the stillness of the night. His social and religious environment has been saturated with belief in the supernatural, as it is usually the case among the Catholic populations of Eastern Europe. We should not wonder, then, that an impressionable child brought up under such conditions would stand in mortal fear of the supernatural and especially of the dead. Now when he was about the age of nine, his mother noticed some prominences on his right chest; she was afraid that they might develop into something serious, requiring, possibly, hospital treatment and even a surgical operation, which the popular prejudice does not favor. It was then suggested to the mother that the hand of a dead person possessed the virtue of blighting life and of arresting all growth, and would therefore prove a “powerful” medicine’s charm” for undesirable growths. It happened that an old woman in the neighborhood died; the little boy was taken into the room where the dead body was lying and the cold hand of the corpse was put on the child’s naked chest. The little fellow fainted away in great terror. One can well imagine what a shock such an experience was to the child. It is from that time that his frightful dreams date. The fear of dead people became subconsciously fixed and manifested itself as an insistent fear of the dead and, in fact, of anything connected with the dead and the world of spirits. It is to the same period that patient refers the onset of his headaches. Another experience, however, entered here and helped to form the complex manifestations of the dreams and the headaches. The patient had hardly recovered from the shock of the “dead hand,” when he had to pass through a still more severe experience. A party of drunken soldiers stationed in the little town invaded his house and beat his father unmercifully, almost crippling him; they knocked down his mother, killed a little brother of his, and he himself, in the very depth of a winder night, dressed in a little shirt and coat, made his escape to a deserted barn, where he passed the whole night. He was nearly frozen when he was found in the morning, crouching in a corner of the barn and shivering with fear and cold. From that time on the headaches manifested themselves in full severity, with deathlike paleness and intense cold of the body. Such incidents have been found in other similar cases, coming from that part of the country where social life is still primitive and is unfortunately disturbed by unfavorable political conditions. However this may be, one thing stands out here clear and distinct, and that is the fact that the various recurrent psychomotor states, otherwise unaccountable, could be referred, by means of the hypnoidal states, to dissociated systems having their origin in a disaggregated subconscious.
X. CASE OF RECURRENT EMOTIONAL STATES. The following case may be of interest from the fact of the insistence of the recurrent emotion which it presents: Mrs. J. A., age thirty-eight. Married. Parents were of nervous temperament. Sister is well. Patient is of Irish decent, born in United States. She had a common school education and is not very intelligent. A physical examination shows the patient to be poorly nourished; she experiences peculiar noises in the right ear, and when she falls asleep she hears occasionally voices. As far as she can remember this persisted since her childhood. Pupils react well to light and accommodation; patellar reflexes are greatly exaggerated. She sees spots before her eyes and has vivid visual dreams. Menstruation normal, regular and not painful. Sensibility to touch, pressure, pain and temperature is in good condition. She has no headaches, no tremors, no motor disturbances. Patient complains of a painful and very distressing sexual affection in the presence of men. The excitement is sometimes very intense and she is then in agony over it. She is ashamed of it and is disgusted with herself, but the feeling is sometimes sweeping over her with such force that she has great difficulty in suppressing it. The “evil and disgusting” thought and feelings torture her and she thinks that death it preferable to such a “miserable” life. She would commit suicide if not for religious fears. The torture of the sexual possession is so intense that she has to shun the presence of men. Curiously enough, it is always the presence of strange men that affects her; the presence of her husband has on her no influence whatever. Even in the church this sacrilegious feeling comes over her and that often in the very middle of the prayer especially when she happens, to be surrounded by men she does not know. She thinks she defiles the church by her impure thoughts and feelings. She cannot be in the company of men on account of those “horrible” feelings over which she has so little control. She is all the more pained by the perversity of her feelings, as she gets affected in the presence of persons whom she would expect least to arouse in her such “abominable” feelings: a priest will excite them and even a negro. Moreover, she somehow has the feeling that in her presence the men who see her seem to experience the same “baneful” excitement; it is a kind of sexual “telepathy.” Occasionally she is seized with unaccountable feeling of fear and is not conscious of what that fear is in particular; she is just afraid and does not know of what,—it seems as if she feels the presence of invisible spirits. By the method of hypnoidization the patient was put in the hypnoidal state. It took some time to quiet her and compose her, as she felt intense anxiety. At last she became soothed and sank into a deep hypnoidal state; but, as it is characteristic of this state, it is varying in its depth from moment to moment and is very unstable. The instability was specially characteristic of this patient, on account of the nature of the case. Still, even under such unfavorable conditions, the hypnoidal state yielded some definite and interesting results, revealing some subconscious systems of experience which gave an insight into the nature of the symptoms. The patient has been a very sensitive and nervous child. She liked to listen with trepidation and shivers to all kinds of stories about spirits, hobgoblins and ghosts, and used to be in mortal fear of goblins. Darkness threw her into great fear, because she suspected the presence of all kinds of mysterious beings and spirits, especially evil ones. She used to hear very strange noises in her ears and was afraid of them and ascribed them to the action of evil agencies. All the dark nooks and corners, cellar and loft and every lonely room and place were peopled by her with ghostly shapes and ghastly figures,—with demons, devils, sprites and gnomes. In her sleep she did not fare any better, since she suffered from frightful dreams and nightmares. The patient thus passed her childhood in continuous fear of unknown and mysterious powers surrounding her on all sides. The child lived in constant terror of things she could not give an account of; she was afraid and did not know of what. It was really a cultivated form of panophobia developed in a timid and nervous child. Later on the fears apparently lapsed, but really did not disappear,—the fears became subconscious. It was those dissociated subconscious fears of something indefinite and intangible of early childhood that were manifested in fully developed womanhood as an inexpressible, unaccountable fear of some impending evil; in short, as panophobia. But how about the sexual affection? In one of the hypnoidal states I at last discovered the subconscious source of the trouble. As a young girl the patient was very emotional, highly excitable, an ardent temperament, with strong passions which she had some difficulty to control. The sexual instinct was awakened rather early and the patient had some difficulty to subdue it. She felt, however, quite safe, as the instinct was kept well under control. When about the age of eighteen she had to return home from a visit to a girl friend of hers. It was late at night; the car she boarded was rather deserted, with only one passenger, a young man, sitting opposite her. Gradually an intense sexual feeling stole over her and seized on her; she felt like one stunned. It seemed to her as if some frenzy got hold of her. The barriers of the pent-up passion evidently seemed to give away. She felt mortified and humiliated at her weakness. At the same time she knew that the man was also sexually affected. She was in agony, and when she left the car the patient was all broken up and prostrated for several days. After a few days she recovered and then the whole incident faded from her memory. The affection, however, really did not disappear,—it only lapsed from personal consciousness; it became dissociated and subconscious, to come once more to the surface of consciousness on subsequent favorable occasions. Thus the hypnoidal states have disclosed the presence of subconscious states, the working of dissociated moments-consciousness in a disaggregated subconsciousness.
XI. CASE OF INSISTENT STATES WITH GYNOPHOBIA. Mrs. C. C., thirty-five years old; married three years. Father is of neurotic, passionate temperament; mother is very nervous, seems to suffer from some kind of epileptiform attacks and periodically from severe hemicrania. Brother and sister are well, though also very nervous and excitable. Patient is quite intelligent, but very emotional,—cries at the least provocation; her attention is easily distracted; mental processes are normal. Desultory memory for numbers and syllables is poor, but logical memory for events past and present is well preserved. There are no perceptual disturbances,—no illusions, no hallucinations. Sleep is light and is disturbed by dreams. Physical examination is negative; except for the fact of marked ill-nutrition and flabbiness of muscles, nothing special could be observed. Patellar reflex is exaggerated. Pupillary reaction and accommodation to light and distance normal. No motor disturbances. She complains of creeping sensations in the extremities, in the hands and legs, also of tingling sensations and numbness in the body and of pains in the back. An examination, however, shows that the patient’s sensitivity to all forms of stimulations is normal. Still at times she suffers much from pains in the back, from paresthesia, tingling sensations and numbness of the extremities and from paresis of the whole body. Motor imitation is very marked, so that the patient frequently copies and imitates motor habits that specially impress her. During the course of her life patient has taken up all kinds of motor habits and twitchings, although she succeeds in arresting them. The motor automatisms are not of an insistent character. What the patient, however, specially complains of is insistent ideas and feelings which torture her, and from which she is unable to free herself. Thus, she has an extreme abhorrence of women. Woman to the patient is impurity, filth; woman to her is the very incarnation of degradation and vice. She would not pass a woman if she could help it. Patient tells me she would not have come up to my office had a woman been standing on the steps. She cannot pass a woman without a sense of nauseating disgust. The house-wash must not be given to a laundry where women work. The patient’s husband corroborated the general symptoms and gave additional data. They had to break up house and remove to another one because carriages opposite their window happened to be hitched in knots and in angles which the patient could not tolerate. Pencils, sticks, books and other objects must be put parallel to the wall and not so as to form an angle or be brought in relation with any of the angles of the room. In kissing her, the husband must be careful that the kisses should not be in a vertical position, nor form any angles, but all must be arranged in rows, parallel to the wall. When dining in a restaurant, should a gentleman and a lady happen to come near them, the table must be immediately left in the very middle of the meal. Patient has certain formulae and phrases which she seems to regard with superstitious awe, although she is conscious of their absurdity. She insists that he husband should repeat verbatim the phrases, and if he happens to substitute another word, or phrases the terms differently, she is much disturbed; he has to help himself out with a dictionary, as she is not supposed to tell him the words. When she attempts to counteract her insistent ideas and impulses, she has crises of crying and of intense depression and suffers agony. Patient feels very unhappy and is distressed over the misery she is in, and of the pain she causes her husband. She bewails her lots, regards herself as insane, but the ideas and impulses are irresistible and uncontrollable. Mr. C. tells me that his wife experiences horror and disgust at the touch, at the mere sight of a woman. He must be on the lookout not to be in one line with a woman, even if the woman be two or three blocks away. Nothing must be picked up on the street, not even the most valuable object, perchance it might have been dropped by a woman. A woman once happened to visit his wife, who could not help herself and had to admit her female guest. The visitor was sent off by some excuse or other. Unfortunately, the woman before leaving stopped on the threshold of the house for a few moments. The house was at once washed, cleaned, scrubbed and purified as after a pest. The husband was not admitted to enter that door for a week, until the threshold was ripped up, another new one made, and the position of the door changed. Patient has also fears, unaccountable fears; she does not now what it is she is afraid of; she is only conscious that, when she remains alone, especially in the evening, a fear suddenly seizes her. The hypnoidal state brought out the fact that the patient, who was educated in a convent, was easily frightened and was specially afraid of the dead and of the devil. While in convent she used to have frightful dreams in which the devil played the chief part. Thus once she dreamed that the devil pinched her ear; she cried out and woke up in great fear. The nun upbraided her, because the devil could not possibly visit such a holy institution as a convent. Once the devil threw her out of bed and threw the mattress after her. The people in the convent became very much frightened and the girls screamed and prayed. The priest was called for and he asked the patient whether she had been praying for the lost souls in purgatory. On being answered in the affirmative the priest advised her not to pray any longer, as the souls from purgatory troubled her. She stopped praying for the lost souls and the trouble completely disappeared. It is the fear of devils and of lost souls that keeps on persisting in the subconscious life of our patient and is now and then giving rise to indefinite fears of the unknown, to panophobia. The foundation of this panophobia was laid in the patient’s tender childhood, and, although she no longer believed in diabolical agencies, in fact even ridiculed them, still the fear did not fully lapse,—it became dissociated and subconscious. The patient’s motor automatisms and imitativeness can be readily traced to her childhood. As a young child patient was very impressible, highly suggestible, more so than any other child of her age,—she suffered then from habit-tics and from choreic-like movements and twitchings. The suggestibility of the patient’s waking state is now greatly reduced, but the subconscious motor suggestions and imitations, so that they do not trouble her much. They are but transient and soon tend to disappear. Some twelve years ago the patient had a bad fall and hurt her spine. It is to that fall the subjective paresthesia in the extremities, the tingling sensations, numbness, paresis and pains in the back can be traced,—the patient passes at each attack through the original experiences of the accident of the fall. When about the age of eighteen the patient suffered a great shock,—one of her near relatives attempted to assault her at night. This accident threw her into a series of attacks which she characterizes as “hysterical attacks.” She really never got fully over it, and the incident, though apparently but faintly present in her conscious memory, has remained active in her subconscious life. The patient’s gynophobia or hatred of women, may be traced to her training received in the convent. While there she was impressed with the belief that woman is a vessel of vice and impurity. This seemed to have been imbued on her by one of the nuns who was very holy and practiced self-mortification. With the onset of her periods, and with the observation of the same in the other girls, this doctrine of female impurity was all the stronger impressed on her sensitive mind. This, however, lapsed from her conscious memory and did not come to the foreground of consciousness until later in life when she was fatigued and exhausted by the strain of office work, toiling many days at a stretch. Still this dissociated, subconsciously buried prejudice of youth might have never come to the surface had not another factor favored its forthcoming and resurrected an experience that had apparently long gone from her active life. Three years ago the patient married a man somewhat younger than herself. Being of a highly sensitive mind and of a suspicious disposition, she developed an intense feeling of jealousy in regard to her husband. It was under these conditions of jealousy that the long-buried and dissociated belief in the impurity of woman came to life again. Curiously enough, instead of applying it to herself, the feeling of gynophobia was applied by her to others. This is due to the emotion of jealousy which called forth that subconscious atavistic belief of the patient’s religious youth. The magic formulae and phrases belong to the same subconscious stratum. The avoidance of formation of angles and the arrangement of kisses had a purely sexual significance.
XII. CASE OF INSISTENT STATES WITH SUBCONSCIOUS TRANSFORMATION OF PERSONALITY. SHERMAN, age thirty-one. Russian. Father is very nervous; mother is also nervous and suffers from severe headaches, so does his sister, who is otherwise quite well. Physical examination is negative; reflexes are normal; memory, attention, recognition, are good; no sensori-motory disturbances. Patient suffers occasionally from severe attacks of headache accompanied by vomiting; he has very depressing nightmares and cries out in his sleep. He is very timid and keeps away from company, communing with himself. In his childhood patient made the round of child diseases. He is physically well, but rather slightly built. Patient is very religious and has “never masturbated.” About the age of eighteen he developed contrary thoughts in regard to God; he could not pray without associating in his mind the words of the prayer with filthy words and curses. Unaccountable fears took possession of his mind. At the same time sexual desires became developed and his mind began to associate them with all kinds of improper relations, even with his sister and with his mother. He is very miserable about these ideas as he is very religious, and the thoughts are not only repugnant to him, but simply torture him by their very presence. Since last year the patient has become worse,—his sexual and contrary religious ideas have become more insistent. The insistent ideas have gained such a hold on the patient that he is distracted with mental anguish, with intense pangs of conscience. He can carry on the work of cigar making with great difficulty, and when he comes back from his work, he sits all by himself and is not doing anything, avoids company and keeps on brooding. Occasionally he gets irritable, cries and claims that the “evil one” has gotten possession of his heart and conscience. He is very nervous, suspicious and gets easily frightened. The mental anguish and the struggle with the insistent “evil” ideas become at times so acute that the patient is like one “crazy”, yells and screams like one possessed. Occasionally he experiences the sensation of some one pulling at his clothes. When on the point of falling asleep he hears “evil” voices. At night, when on the point of waking up, he is tortured by fearful nightmares, cries and moans before he can arouse himself, or be aroused. Patient wants to leave the city, wants to get away from himself, wants to commit suicide. What keeps him back is his intense religious belief. The insistent sexual ideas have taken such a hold on his mind that patient is afraid to remain alone with his sister and even with his mother. In one of our conversations the patient was asked the reason why he troubled himself about the thoughts when he was fully conscious that they were but nonsense, he replied: “I cannot help it; my head gets depressed and heavy; I should prefer to be in hell than to have this kind of nonsense. When I have these ideas my head is dark; all looks dark. When I attend to my natural wants I think of God and associate Him with it to anger Him. When I spit, for instance, I cannot help thinking ‘I spit on God.’” Patient has bad nightmares. He feels that something is lying on him and pressing him; he is afraid of death. He has his eyes open, but he cannot move. On falling asleep, or rather when he finds it difficult to fall asleep, he can hear voices distinctly. The voices talk to him as one man to another; he cannot remember what the voices say. He can hear the voices near the ear, not inside. When patient walks in the street “dreams come to him,” then he seems to wake up and does not remember anything. When he goes to bed he talks to himself and is even conscious that he answers questions. When he wakes he sometimes is under the impression that the “evil one” has gotten a firm hold on him. There is some one, the evil one, who laughs and jeers at him. When a boy of fifteen, he used to have very vivid dreams, could hear steps of “spirit people” in the room. He used also to be frightened by shadows, a fear which dates far back to his early childhood. When about the age of twenty he was pursued by the idea of death, though not of suicide, represented to himself the angel of death very clearly, and the fear made him feel faint. Last summer, to counteract the sexual thoughts and excitement, he attempted to revive the image of the angel of death in order to feel faint, but he did not succeed. About six years ago, patient worked on the sewing machine; one day he suddenly lost the power of movement in the legs. This paralysis lasted three days. He improved and went to his work. Two years ago patiently suddenly lost the use of the right hand and right leg. It was not so much an actual paralysis as an intense pain in moving the leg and hand. He could not raise the elbow and dragged the leg. This lasted from April, 1900, to February, 1901. A year ago a young girl came to visit the family and was placed to sleep in the adjoining room. This developed an intense sexual excitement, with thoughts of sexual character. When this developed, the pain and paralysis ceased. One was substituted for the other. When one trouble began, the other disappeared. The sexual thoughts are accompanied with “burnings” which cause the patient great sufferings. These thoughts come periodically. The evil and “nonsense” thoughts are almost always present and give him no rest. Patient feels dazed; does not know where he is, what he is doing, whether he lives at all. Everything is “like nonsense.” His hypnagogic and hypnapagogic hallucinations consist of very ugly faces of women, of images of women without hands and feet and of other grotesque visions. The insistent ideas are somewhat like “voices”—they call him names, they laugh at him, at his religious beliefs, at all that he regards as moral and sacred. He feels that there is another person in him that instills in his mind those evil ideas against everything that is holy. The more he fights the more that evil person confuses his thoughts with “unholy ideas,” and finally even paralyzes his body. Patient can read well “profane writings,” such as newspapers, novels, but a religious book, and especially the scriptures, awaken in him the evil one who makes him suffer untold agonies, intolerable pangs of conscience. I may add the following interesting letter written to me by the patient: “I give a short account of my life so as to help the doctor to form an idea of my condition. I hope you will pardon me for putting you to so much trouble. “In my early childhood and youth I suffered a good deal and many times I had to go without food. When I was about fourteen, I lost two brothers, one younger and one older than myself. The younger brother, a boy of three, I used to take care of and instructed him. I loved him than my own life. Besides, my parents were at that time in very bad circumstances. I was greatly upset and felt deprived of bodily and mental strength. “I began at that time to learn the trade of jeweler but as my mind was very weak I could not do the work, and after ten months of great suffering I fell sick and had to give up the work altogether. “I then obtained a position as clerk in a small store and had trouble. I have suffered greatly and still continue to suffer. You can see, therefore, that up to the time of my coming to this country I have suffered greatly and still continue to suffer. “I shall now describe the silly, evil thoughts that torment me so fearfully. “When I was eighteen years old it suddenly occurred to me to curse the Creator. The curses were awful. Since then my personality has changed. Intense sexual passion took possession of me with frequent nocturnal emissions. Confusion came into my mind. Evil thoughts got hold of me. I began to substitute contrary sentences; thus, instead of ‘The earth is full of His glory,’ I substituted ‘The earth is full of his filth.’ During prayer these thoughts would come to me. The most indecent filthy thoughts would come to torment me. I would cry for hours and struggle against them, but of no avail. The more I tried to drive those thoughts from my mind, the more persistent and unholy would they become. Since then I have become depressed and melancholy. I have lost all desire for life. I feel as if I would like to go into a desert and there die. I want to live and have a quiet undisturbed mind. I am a human being; I cannot hide myself. I have eyes and ears, but everything I see and hear is transformed into evil. “I cannot undertake to describe all the bad thoughts that enter into my mind. If you could drive all this nonsense from my mind without weakening my love for my people or my religion, if you could bring it about that I could read the Bible without changing the thoughts into evil and my mind should be clear, you would save my life. Oh! if light should dawn upon me and my mental darkness should disappear! “I have confessed to you everything, more than I would to my father and mother.” The condition of this case can be understood in the light of the patient’s childhood, revealed by means of various intermediary states and by means of indirect inquiry of the patient’s parents and sister. The patient passed his childhood and youth in extreme poverty and misery, in the midst of social, political and religious oppression. Living from his very babyhood in misery, extreme poverty and squalor, often enduring cold and the pangs of hunger, surrounded by disease, sufferings, pains due to starvation, by sickness and death of those near and dear to him, the patient, with all his natural intelligence, had been fostered ins the strict religious belief of a beneficent Providence. The contrast between the ideal Providence and the real misery was too great. With all his needs, desires and instincts suppressed, thwarted and mocked at by the merciless conditions of life subconscious protests began gradually to form in the patient’s mind; the protests, gathering force, finally burst forth with the crisis of adolescence. It was a protest of subconscious mental activity against a life of misery hallowed by religion. It was the protest of the subconscious against the teachings of religion, a subconscious revolt against Providence and all the religious and moral institutions. Out of the chaos of discordant, dissociated elements we see the formation of an ill-shaped, maimed, but defiant subconscious secondary personality of nihilistic tendencies,—a state through which his country and countrymen are now passing. We witness here a struggle full of anguish and agony between a shattered personality and a newly-forming self out of a chaotic disaggregated subconscious. Like the demoniacal possession of the Middle Ages, it is the reading of the sacred scriptures that throws the patient into a condition of distress and of inner combat of the discordant elements. The patient is not fully aware of the why and wherefore of the “pangs of his conscience,” but still he seems to have some dim suspicion of the nature of his malady, when he asks for help “without weakening my love for my people and my religion.” The patient’s condition is the agony of a mortally wounded self struggling against the merciless onslaughts of a pitiless, nihilistic secondary self forming out of chaotic states of a disaggregated subconscious.
XIII. THE MOMENT THRESHOLD AND DYNAMOGENESIS. In concluding this paper it may be well to point out some principles, important in many respects, but which at the present moment are of interest from a psychopathological as well as from a practical therapeutic standpoint. Living tissue can only be set into activity by stimuli of certain minimal intensity; should be the stimulus fall below that minimal intensity, the living protoplasm will not react. This holds true of all cells, from the lowest to the highest,—from the bacterium and infusorium to the highly differentiated cell, such as muscle cell or neuron. The reaction of the living protoplasm to the stimulus shows the irritability or sensitivity of the cell. This sensitivity has its physiological threshold, so that a stimulus falling below a certain intensity cannot call forth any reaction in the cell. The rise or fall of the threshold would mean an increase or decrease of the minimal intensity of the stimulus requite to bring about a cellular reaction. By varying the conditions of sensitivity, such as mechanical, thermal, electrical, chemical and nutritional, the physiological threshold can be raised or lowered. The same holds true of a whole psychophysiological system,—there is a threshold of sensitivity below which the minimal stimulus cannot fall, the latter will not awaken any reaction in the system. All the senses reveal the presence of such thresholds which are also present in the case of all the higher psychophysiological systems. If we term the stimulus which can just bring about a reaction in the system the stimulus threshold, we can say that a given system can only be thrown into activity by a stimulus rising in intensity above the stimulus threshold. Intensity of stimulus, then, is an indispensable condition of the functioning of a psychophysiological system. In highly differentiated cells, however, it is not only the quantity or intensity of the stimulus that is to be considered, but also the quality. The visual sense organ is not affected by auditory stimuli nor can the auditory sense organ be affected by visual stimulations. Similarly, in the functioning of the higher psychophysiological systems the quality of the stimulus should not be overlooked. Systems that remain inactive under one set of stimuli, however intense, will respond to another set of a different quality. The same holds true of that synthesis of mental systems which we term moment consciousness. To set the moment into activity, the moment threshold must be passed, and not only the intensity of the stimulations should be taken into consideration, but also the qualitative aspect of the stimuli. Ideas, emotions and feelings which apparently remain dormant at the action of one set of excitations will respond readily to the action of excitations of a different nature. Habits, habitual movements, habitual thought, depend entirely on the qualitative character of the excitations, on the combinations of special objects, circumstances and times. It will take too much place to develop here this principle, as we expect to work it out in full elsewhere. Meanwhile, we can simply point out here that the quality of the stimulus is one of the important factors in the activity of a psychophysiological system, or of a moment consciousness. Besides those two factors of intensity and quality, another factor, that of inhibition, plays quite a role in the variations of the threshold. We are acquainted with inhibitions in physiology, such, for instance, as the inhibitions exercised by the pneumogastric nerve on the heart, or the arresting of the activity of glands or of the peristalsis by the stimulation of afferent nerves. We know also of central inhibitions, such as fear, distress, pain, acting as so many inhibitions on the peripheral organs and serving to arrest functioning activity. Similarly in mental life, complex as it is, the highly organized psychophysiological systems, with their concomitant moment consciousness, still fall under the same general physiological laws of inhibition. In the course of associative activity systems and moments become organized into more complex groups, into more complicated systems or constellations of systems which, to maintain their functioning equilibrium, keep one another in check or under inhibitions. Such a formation of checks and inhibitions is just what takes place in the training and the education of the individual and the race. After psychophysiological system or moment entering into relations with other systems and moments is bound in the course of its associative activity to form inhibitions to its function by the direct influence of external or internal excitations. In other words, there is a rise of threshold due to inhibitory associations. Inhibition and rise of threshold may also result in a different way in the process of association. We may possibly law it down as a law, which plays no small role in the interaction of systems and moments, that in a series of aggregation of various systems or moments, forming a more complex organized whole, due to association and synthesis of the component systems, having various thresholds, the ones having the higher thresholds will raise the thresholds of the moments having a greater sensitivity. This, however, may be counterbalanced by the lowering of the moment threshold by associations with moments of great sensitivity, that is, with low moment thresholds. While on the one hand the inhibitions and the consequent rise of threshold go along with the complexity of systematic structure and as well as with the increase of associative activity, both in extension and intension, there is at the same time an advantage gained for the system, inasmuch as it really has now more chances to become active on account of the greater number of systems with which it has become associated. The threshold of the associated system rises, but on the other hand, the chance for activity increase, while the liberation or discharge of energy with the consequent evil effects of extreme fatigue, exhaustion and ill-nutrition are checked and guarded against by the inhibitions and the rise of threshold. What happens now when a psychophysiological system becomes dissociated? The inhibitions become removed and the threshold falls. The system is no longer checked by inhibitions or by other systems, and hence, with a lowering of the threshold, becomes sensitive, reacting to any slight, passing stimulus, manifesting or liberating all the energy it possesses until fatigue and complete exhaustion set in. From this vantage ground we can understand the fact of the extraordinary energy which the dissociated subconscious systems manifest, so much so that the unusual energy appears almost supernatural and has on that account been ascribed by the superstitious to diabolical possession. To quote from a former work of mine: “When a system present in the upper personal consciousness is to be disintegrated, the suggestion given should be kept out of the patient’s personal memory. One can observe this fact clearly in post-hypnotic suggestions. If a post-hypnotic suggestion is fully remembered, it usually miscarries,—the suggestion loses its efficacy and often comes up as a word-memory without the stringency of realization. When, however, amnesia is enforced, the post-hypnotic suggestion is fully realized. A dissociated system present in the subconscious, when coming to the surface of the upper strata of consciousness, becomes manifested with intense sensori-motor energy. Dissociation gives rise to greater dynamogenesis. This principle of dynamogenesis is very important, and cases of so-called impulsive insanities and ‘psychic epilepsy’ are really due to this cause. “A system entering into association with other systems is set into activity, not only directly by its own appropriate stimuli, but also indirectly through the activities of the various systems associated with it. These associative interrelations bring about an equable and normal functioning activity, controlled and regulated by the whole mass of associated systems. The mass of associated systems form the ‘reductives’ of each individual system. In dissociated systems the controlling influence of the ‘reductive mass’ is lost and the result is an over-activity, unchecked by any counteracting tendencies. “This relation of dissociation and dynamogenesis is closely related to periodicity of function, with its concomitant manifestation of psychomotor activity characteristic of all passions and periodically appearing instincts. Dissociated systems present impulsiveness, because of lack of associated counteracting systems. The only way to diminish the overpowering impulsiveness with which the dissociated subconscious systems make an onset in their rush into the personal consciousness is to bring about an association, to work the dissociate systems into the tissue of the patient’s consciousness. “Physiologically, it may be said that a neuron aggregate, entering into association with other aggregates and being called into activity from as many different directions as there are aggregates in the associated cluster, has its neuron energy kept within the limits of the physiological level.6 A dissociated neuron aggregate, on the contrary, is not affected by the activity of other aggregates; it is rarely called upon to function and stores up a great amount of neuron energy. When now an appropriate stimulus liberates the accumulated energy, the activity is overwhelming and is very much like the eruption of an underground volcano, giving rise to temporary attacks, to ‘seizures’ by subconscious states of the whole field of the upper consciousness,—‘seizures’ which, being really of the nature of post-hypnotic automatisms are generally mistaken for epilepsy, the attacks being regarded as epileptic manifestations, as ‘larval epilepsy,’ as ‘epileptic equivalents,’ as ‘psychic epilepsy.’ With the restoration of the equilibrium of the neuron aggregate, with the synthesis of the associated systems, a synthesis which can be brought about by different methods, the subconscious eruptions, the attacks, or ‘seizures’ vanish, never to return”.7
XIV. THE PRINCIPLE OF RESERVE ENERGY. We have pointed out the significance of inhibitions in keeping back the systemic neuron energy from fully being discharged under normal conditions of life, and we have also shown that the removal of inhibitions results in the full liberation of the accumulated neuron energy. This fact, so striking in the domain of recurrent psychomotor states, almost forces itself on the attention of the student of abnormal psychology. From such a fundamental fact of abnormal mental phenomena, we may draw some conclusions in regard to mental life in general. For, after all, the laws of pathology do not differ from those of physiology in general, the pathological really being the physiological under special conditions. The normal is either the usual, the habitual, the customary, or is, at best, an ideal construction of the variations of life more or less successfully adjusted to the conditions of the external environment. This adjustment, however, keeps on constantly shifting ground, continually changing the relative position of the normal and the abnormal. From this standpoint pathology is of the utmost importance in the study of organic life. The pathological being the normal out of place, the so-called normal under special conditions, pathology that deals with the abnormal gives us a deep insight into the general laws of normal physiological activity. All the experiments in physiology consist practically in the production of so many pathological conditions and states. When the physiologist makes injections, sections and stimulations by various agencies, what else does he effect if not the production of the pathological, in order to learn the physiological action of the various tissues and organs? In our psychopathological study we have really followed the interrelations of mental phenomena under special conditions; it is the physiological method of experimentation by production of pathological variations; the conclusion arrived at in psychopathology should apply to mental life in general. What is this conclusion? It is the principle of potential subconscious energy or, more briefly stated, the principle of reserve energy.8 The moment thresholds of our moment consciousness, or, put in physiological terms, the thresholds of our psychophysiological systems, are usually raised, mental activity working in the course of its development and growth of associative processes under ever-increasing inhibitions with ever-higher thresholds. It is enough to compare the educated, the civilized, with the uneducated or with the barbarian and the savage, to realize the truth of our statement reached from a study of psychopathological facts. On account of the threshold and inhibitions, not the whole of the psychophysiological energy possessed by the system or moment is manifested; in fact, but a very small portion is displayed in response to stimuli coming from the habitual environment. What becomes of the rest of unused energy? It is stored, reserve energy. Biologically regarded, we can well see the importance of such stored or reserve energy. In the struggle for existence, the organism whose energies are economically used and well guarded against waste will meet the better success in the process of survival of the fittest, or will have better chances in the process of natural selection. The high thresholds and inhibitions will prevent hasty and harmful reactions as well as useless waste of energy, unnecessary fatigue and states of helpless exhaustion. Moreover, natural selection will favor organisms with greater stores of reserve energy which could be put forth under critical conditions of life. In fact, the higher the organization of the individual, the more varied and complex the external environment, the more valuable and even indispensable will such a store of reserve energy prove to be. The course of civilization and education, by continuously raising the thresholds and inhibitions, follows the line of natural selection and keeps on increasing the disposable store of potential subconscious or reserve energy both in the individual and the race. It is in this formation of an ever-greater and richer store of disposable, but well-guarded, reserve energy, that lies the superiority of the educated over the uneducated and the supremacy of the higher over the lower races. Civilization and education are processes of economy of psycho-neural force, savings of mental energy. But what society is doing in a feeble way natural selection has done far more effectively. What education and civilization are doing now on a small scale and for a brief period of time the process of survival of the fittest in the ever-raging struggle for existence has done for ages on a large scale. We should, therefore, expect that the natural reserve energy would far exceed that of the cultivated one. The brain and mind of the ancient German differed in nothing from his modern descendant, the German professor, and still what a difference in the manifestation of mental energy. The savage brain and mind do not differ from those of their civilized descendants, and still what an ocean of mental life separates the civilized man from his savage progenitor. It is against the evidence of biological sciences to suppose that the acquisitions of the cultivated brains have actually been transmitted from generation to generation. It is not likely that acquired characteristics brought about by social life will change so radically the brain in the course of some forty or fifty generations that separate the civilized man from his savage progenitor, and the trend of biological evidence hardly favors the transmission of such acquired characteristics. “There sits the savage,” once exclaimed an eminent pathologist, “with three quarters of his brain unused.” Yes, there sits the savage with a brain far surpassing the needs of his environment, harboring powers of a Socrates, Plato, Aristotle, of a Shakespeare, Goethe, Darwin and Newton. The ancient German and Briton hardly differed in their mental powers from their contemporaries, the civilized Egyptian and Babylonian. What, then, did those Aryan savages do with their richly endowed mental energies? Nothing. The mental energy was lying fallow,—it was reserve energy,—energy for future use, for the use of future ages of coming civilization. But what about the cultivated man? Does he suffer from neurasthenia, from nervous impotence, because, as some would have it, on account of the strain of civilized life he has exhausted his store of nervous energy? One may well ponder over the significant fact that it is the neurasthenic, the “psychasthenic” who is doing the world’s work. We must remember that civilization is but of yesterday and that the reserve energy is hardly touched upon. In the treatment of the phenomena of psychophysiological dissociation, in the protean symptoms of nervous and mental exhaustion we should not forget this biological principle of reserve energy and should make attempts to use it. In many cases the inhibitions become too heavy and the thresholds too high. We must loosen the grip of some of the inhibitions and lower the thresholds, thus utilizing a fresh supply of reserve energy. It is certainly a great pity that the medical schools have until now ignored the whole domain of psychopathology and have left psychotherapeutics in the hands of the superstitious and the unscrupulous,—of the mental healer and Christian scientist. Medical colleges are justly proud of their laboratories, but thus far not a single medical school has considered it important enough to establish a psychopathological laboratory. Is the study of the phenomena of abnormal mental life of little or no consequence to medical science? Unusual combinations of circumstances, great radical changes of the environment, often unloosen the inhibitions and, overstepping or lowering the thresholds, release some of the reserve energy. Critical periods, great dangers, wars, revolutions, often make man rise to the occasion, so that apparently insignificant and worthless individuals display an energy unforeseen and unsuspected and which makes of them heroes and heroines. There is a rise in intensity and a qualitative change in the stimuli, an unloosening of some of the inhibitions with a consequent release of some of the bound-up reserve energy. In this respect wars and revolutions may be regarded as important factors in the manifestation of human potential energy. The Persian and Peloponnesian wars unloosened some of the energies of Greece, giving rise to great thinkers, scientists and artists, having a lasting influence on the destiny of humanity. The constant wars and national misfortunes of the Jews released their reserve energy and made them a race of prophets, apostles and martyrs, deeply affecting the course of human civilization. What about the wars of Reformation, with which opens the new era of the free development of modern European civilization? What about the English, American and French revolutions which have released new supplies of energies and have opened a new arena for the free development of political, social and industrial forces? In our own times we meet with the example of the Japanese, who, under the strain of great national danger, have released a reserve energy unsuspected in races of the Mongolian stock. Reserve energy becomes manifested under the influence of radical changes in the environment, just as we have found that psychophysiological systems react and start into function under the influence of special conditions and special appropriate qualitative stimuli. In the therapeutic treatment of functional nervous and mental diseases, in the treatment of neurasthenia, or psychasthenia, hysteria and insistent or recurrent mental states, the physician should fall back on this natural stored-up reserve energy. I find this principle specially successful in my treatment of so-called functional and habit psychoses, in various forms of insistent psychomotor states, in the whole domain of mental dissociations, and in cases of alcoholism where an almost complete moral transformation of the personality is observed through the liberation of some of the patient’s subconscious reserve energy.9 The method of hypnoidization with is induced hypnoidal states may help out in reaching this source of reserve energy. The hypnoidal states, being intermediary in character, form a common meeting ground of the conscious and the subconscious, and it is in these states that we often can catch glimpses of the individual’s stored-up energy. By means of special qualitative stimuli and by the reduction of the inhibitions and of the moment thresholds we are able to utilize energy out of the patient’s reserve energy for the reestablishment of disturbed inner relations and dissociations. The Hanna case as well as many other cases have been practically treated by me on this principle by means of the hypnoidal or intermediary states [see also Multiple Personality]. Most of my work is now being carried out on these lines. The hypnoidal states may be modified, the methods of their induction may be varied, and again the whole method of treatment may be carried out on different lines, according to the nature of the case and character of the individual, but all the variations in the method of treatment are based on one fundamental principle,—the principle of reserve energy. For, as one studies mental life with its infinite variety of mental dissociations and subconscious activities, one becomes more and more impressed with the fact that beyond the psychophysiological limits of energy, available for the habitual adjustments to the ordinary external conditions of life, there is a vast store of reserve energy whose depths one cannot gauge,—but
["The chalice of this realm of spirits
________________
1
Psychopathological Researches;
Multiple Personality.
W. J. Sidis Archive Boris Sidis Archive Menu
|