|
I In the diagnosis and treatment of various maladies that come to the knowledge of the physician, the mental factor is the most elusive and the most apt to he ignored by the busy practitioner. It is high time that the medical profession should awaken to the consciousness of the importance of mental activities on bodily functions and not let the Mental Healer, the Christian Scientist, the New Thought practitioner and the charlatan handle and treat human ailments which should be alleviated and helped by the skill and knowledge of the physician guided by scientific research. Although the subject of the relation of mental and physical functions is by no means new, still, considering the fact that few medical men realize its importance and fail to understand clearly the scientific basis on which it rests, we may call attention of the medical man to the mental functions of the human organism, functions which are often overlooked by minute, scrupulous physical diagnosis, often ignored and even treated with contempt, especially by the young practitioner, under the disparaging term of "imagination." The influence of mental states on bodily functions has been known a long time back in the very early stages of man's development. Instance the influence of the medicine-man with his magical incantations among savage and barbarian races, the power of the priest in antiquity and the middle ages, a power still persisting in our own times in various disguises, such as the Lourdes and other miracles of like kind. The Mental Scientist with his metaphysical treatment, the Christian Scientist with his silent prayers and "absent" treatment are but echoes of the past, remnants of superstitions, based on the fundamental but little understood fact of the influence of mental states on bodily functions. The ancient nations, the Egyptians, Babylonians, Assyrians, Greeks and Hebrews were familiar with the fact of mental suggestion. There is in the British Museum a tablet found at Thebes representing a priest hypnotizing a patient. The biblical story of the brazen serpent that cured those that gazed at him points in the same direction. Cures by hand manipulations strikingly similar to the method of modern hypnotists were performed in the temple of Isis, Osiris and Serapis. In the Greek temples of Æsculapius, diseases were cured by having the patient fall into deep sleep. This practice was kept up during the period of Roman civilization. With the rise of christianity this mode of treatment was condemned by the church, but really indirectly practiced by the priests and the saints. It remained for modern times to make a scientific study of the matter by subjecting the phenomena to a rigid investigation.
II The influence of the central nervous system, or rather of the cortex with its mental processes on bodily activities and especially on visceral functions is a phenomenon of every day occurrence, such as the loss of appetite, of change of heart beat, of the pulse in the case of fright, of bad news, or in the case of good news, of contentment and joy, As Darwin puts it, "The manner in which the secretions of the alimentary canal and of certain glands, as the liver, kidneys or mammæ, are affected by strong emotions is another excellent instance of the direct action of the sensorium on these organs." The heart which goes on beating night and day is extremely sensitive to external stimulations. Claude Bernard has shown how the least excitement of sensitive nerves reacts through the pneumogastric nerve on the heart. The vasomotor system is directly acted on by the sensorium as we see when a man blushes from shame. "In the case of hunger or of desire for tempting food the mouth waters,"1 that is, there is an abundant secretion of saliva. It has been observed by early investigators (Bidder, Schmidt and Richet) that the sight of food also causes the secretion of gastric juice. Pavlow in his experiments showed that the central nervous system acts on the secretion of the stomach through the vagi nerve, that innervate its glandular activity. He made a gastric fistula in the animal (in the dog), then exposed the esophagus, opened it and sewed the cut end together to the edges of the wound. Food taken by the mouth fell out through the opening, but an abundant secretion of the gastric juice was observed. After division of the vagi the reflex secretion ceased. There are two moments which cause a secretion: (1) the psychic moment, the desire for food and the sense or satisfaction and (2) the chemical moment; the psychic moment is the more important. We may give here a more detailed account of the remarkable experiments carried on in Pavlow's laboratory. By the term "unconditional reflex," Pavlow means to indicate the response which the animal with a fistula in the secretory glands, such as the salivary glands, for instance, reacts by secretion of saliva to a stimulus coming within the experience of the animal, such as bread, meat and other foods. By "conditional reflex," Pavlow indicates the reaction made by the operated animal, to a stimulus artificially associated with the unconditional reflex. Thus, during the time the animal is fed, a light is flashed or a whistle is sounded. After a series of repetitions, twenty, thirty or a hundred, the animal reacts with secretion of saliva to that artificially associated stimulus, such as optical or auditory. Now here comes the specially interesting work of Pavlow and his collaborators: When another stimulus is in its turn associated with that of the conditional reflex, the result is not an increase, not an indifference to, but a total inhibition of the conditional reflex. Vasiliev, working in Pavlow's laboratory, associated the sound of a metronome with the conditional reflex of a scratch stimulus. He finds that the process of inhibition runs in three phases for intense associated stimuli and in two phases for weak ones.
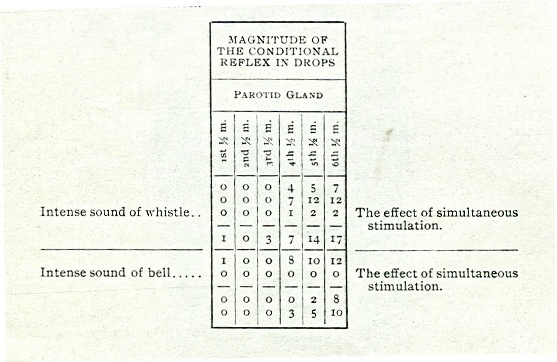
Savadsky2 has modified the conclusions of the previous investigators, but he affirms the fact that an intense sound, completely annihilates the secretion due to scratch-stimulation. While a weak stimulus, a weak sound produces a lesser effect. He finds that the external stimulus disturbs or inhibits the condition of the nerve centers, inhibits the condition which is predominant at that moment, stimulating the inhibitory stage and inhibiting the excitatory stage; in other words inhibiting whatever process is at that moment taking place. The following tables showing the inhibitory influence of intense stimulations associated with the conditional reflex may serve as an illustration. The conditional reflex is formed from a scratchstimulus, intense whistle, or intense sound of bell as simultaneous extraneous stimulation.
In summarizing the work of previous investigators in Pavlow's laboratory, Orbeli says: Vasiliev and Mishtovt have shown that any phenomenon indifferent in itself may not only become a source of a new conditional reflex, but may become a special inhibitory agent in relation to the existing conditional reflexes; it is only requisite that the phenomenon should be repeatedly associated with the conditional reflex in such cases when the latter is not reinforced, that is, when not accompanied by the conditional reflex. If, for instance, phenomenon A coincides in time with the unconditional reflex of the salivary gland, the phenomenon A becomes a source of conditional salivo-secretory reflex. If, however, in cases when A comes separately without the unconditional reflex, a new phenomenon B is associated with A, B gradually becomes a source of inhibition of the conditional reflex. The relation formed is such that A by itself calls out a secretion of saliva, while in association with B does not call out any saliva; that is, B inhibits the action of A. That phenomenon is termed in Pavlow's laboratory 'conditional inhibition.' B is the conditional inhibition in relation to the conditional reflexes on A. This quality of the nervous system to work out special cases of inhibition makes the conditional reflexes an extremely delicate and perfect index of reactions of the organism to its external environment. The animal reacts only to those phenomena which really coincide with that or other specific stimulation and serve as signals of the latter. When, however, an extraneous stimulus becomes associated, a stimulus which serves as a signal of unreality of the nervous phenomenon, the reaction becomes arrested and the organism thus rids itself of fruitless labor." On the strength of his own experiments performed on the visual reflexes of the dog, Orbeli comes to the same conclusion with Vasiliev and Mishtovt, Babkin and Savadski, "that every phenomenon which coincides with the conditional reflexes in all cases when the latter is not accompanied with the unconditional reflex becomes an inhibition in relation to that same conditional reflex."3 Similarly in the experiments carried on in my laboratory, I find that when a galvanic deflection is brought about by a specific stimulation of painful character, the co-existence of another stimulation is apt to decrease the magnitude of the galvanic reflex. If the stimulation be a pinch, a prick or a snap on the skin or on the nose, the simultaneous association with a different stimulation coming from another source, such as intense sound, a loud shout, tends to act as an interference as an inhibition, decreasing the magnitude of the deflection and increasing the latent period of the galvanic reflex. Furthermore, the expectation of the disagreeable or painful stimulation is associated with a stimulation coming from a new extraneous source. the result is not an increase, but a decrease, of the magnitude of the reflex, with an increase of the latent period. In many cases the decrease may amount to a total inhibition of the deflection. The more complicated those new associated stimulations become, the weaker is the galvanic reflex in response to the painful stimulation. Thus, if the expectation of a snap on the nose be simultaneously associated with a loud shout or with another intense stimulation, to which the patient does not react with any emotional excitement, the galvanic deflection to the original disagreeable stimulation becomes considerably diminished and even totally abolished, On the other hand, the magnitude of the galvanic reflex becomes enhanced, while the latent period becomes shortened with the exclusion of external stimulations. such as closure of eyes and complete repose.4 Experiments clearly prove that there is an intimate relation between emotional states, mental effects with their pain-pleasure tone on the one hand and motor reactions on the other, as indicated by "the galvanic phenomenon."5, 6
III An intimate relation exists between the functions of the central nervous system on the one hand and the sensory, motor and visceral functions on the other. This vital relation, though unobtrusive in the normal individual, stands out clear and distinct in the whole domain of functional diseases. Clinical and laboratory studies have brought to light the important fact that all those cases that go under the description of nervous disturbances of a functional character, such as hysteria, hystero-epilepsy, the so-called larval epilepsy, psychic epilepsy, neurasthenia, psychasthenia, and all the forms of the neuroses and phobias in regard to external and internal stimulations are all to be ultimately referred to mental disturbances, whether conscious or subconscious. All such disturbances are termed by me psychopathic diseases or functional psychosis. Such psychopathic maladies may be purely ideational and emotional or they may he of the character of physical disturbances affecting the various sensory organs-motor activities or visceral functions. If the predominating symptoms are ideational and emotional, the symptom-complex is a psychoneurosis; if, however, the predominating symptoms are of a sensory, sensory-motor, or visceral character, then the symptomcomplex is a somopsychosis. Both psychoneurosis and somopsychosis are essentially psychic in origin.
IV Perhaps we may take occasion here to make a brief differential diagnosis between the two main varieties of functional psychosis, psychoneurosis and somopsychosis. Such differential diagnosis is of the utmost importance not only from a purely scientific medical standpoint, but it is of clinical consequence from the standpoint of treatment. The pathognomonic characteristics or symptoms of psychopathic diseases or of functional psychosis are: 1, Dissociation of mental systems and functions which may have, but generally has not as its foundation any corresponding anatomical distribution of structure; 2, Cyclical occurrence of attacks, exacerbations and relaxations associated with fluctuations of emotional disturbances, often preceded by a vague form of brooding and followed by periods of worry and depression; 3, Subconscious formation of ideas and emotions of which the patient is vaguely aware or even completely unaware; 4, Infantility of the subconscious formation; the subconscious ideas and emotions can be traced to child experiences and infantile formations of mental systems falling outside the synthesis of the patient's normal adult personality; in other words, there is a formation of parasitic personalities, engrafted from early childhood on the main trunk of the patient's individuality; 5, Conscious loss and the subconscious gain; in psychopathic diseases the loss of a function is only in consciousness, in so far as it is lost from the direct consciousness of the patient, subconsciously the patient is found to be in full possession of the lost function: many methods have been elaborated in psychopathology to demonstrate the presence of the affected or of the lost function; moreover, the function is even found to be exaggerated and intensified in the subconscious. This may be regarded as the paradox of psychopathic diseases or of functional psychosis. 6, A distinct impairment of volition is present in all forms of functional psychosis. There is hesitation, doubt, the inability to perform a function dependent on the belief of such incapacity and on the thought firm1y fixed in the patient's mind that such activity is impossible, or that a given derangement of function is the make up of his life and organization. He suffers from weakness of will power. There is little initiative in the patient, though he is whimsical, capricious, asking for change. A real fundamental change he has not the power to effect, in fact, he shrinks from all radical changes made in his life. On the whole, we may say that recurrence of dissociative states is pathognomonic of functional psychosis in its main divisions, psychoneurosis and somopsychosis, so much so that we may designate such conditions as recurrent mental states, which are on that account often related to epileptic seizures of the psychic type. This is especially the case with the more violent manifestations of the sensory-motor varieties. The definition, then, of functional psychosis or of psychopathic diseases is a disturbance of functions, ideational, volitional, sensory, motor and visceral due to abnormal mental states. The symptomatology briefly stated is dissociation, recurrence, well developed subconsciousness, absence and presence or loss and gain of functional activities.7
V The symptoms manifested in psychopathic maladies are protean in form: 1. Motor and sensory-motor attacks may be present, symptoms of trembling, shaking, paresis, paralysis, rigidity, disturbances of locomotion and of muscular co-ordination, such as contractures, convulsions, catalepsy and lethargy, whether general or localized. 2. Sensory disturbances may be present, such as anesthesia; paresthesia, hyposthesia, analgesia, paralgesia, and hypolgesia; akinesia, parakinesia and hypokinesia, various forms of loss of muscle-sense and kinesthesia. 3. Respiratory disturbances may occur, as coughing, hawking, apnea, dyspnea, asthma and generally affections of the respiratory passages, among which hay fever is not infrequent. 4. Cardiac affections are often present, such as precordial pain, palpitation, bradycardia, tachycardia, cardiac arrhythmia and the well-known false angina pectoris. 5. The most common disturbances arc vasomotor, trophic and gastrointestnal,―the stomach is deranged, there is pain in the abdominal regions, vague fugitive soreness all over the abdominal region or in special places, nausea, vomiting, bulimia and anorexia, complaints of indigestion, irregular or obstinate; constipation; irregular or persistent diarrhea. 6. Renal disturbances are not uncommon, such as anuria and polyuria. 7. In women the functions of menstruation often become affected and we may find conditions of dysmenorrhea, amenorrhea, menorrhagia and various disturbances of the Fallopian tubes, ovaries and uterus. 8. The central nervous system, especially the brain, may be often involved, and the symptoms presented are headaches, general and localized; migraine, the so-called clavus hystericus, pains in the back of the head, backache, dizziness, vertigo and a general feeling of incapacity and fatigue. 9. On the mental side there are all forms of disturbances, such as perceptual, illusions and hallucinations; conceptual, such as insistent ideas; fixed conceptual systems, disturbances of attention and memory, such as aprosexia and the various forms of amnesia; disturbances of will, sex and personality.8 The limitation and scope of the present paper do not permit me to go into details of the subject.
VI The differential diagnosis between somopsychosis and psychoneurosis may be made by the fact that in somopsychosis the physical or organic symptoms predominate, while in psychoneurosis the mental symptoms are mainly evident. In the somopsychoses the patient complains of physical symptoms, such as stomach and intestinal disturbances, contractures, convulsions, anesthesia, paresis and paralysis of various organs. It is for the physician to find the underlying subconscious psychic states. In the psychoneuroses the patient complains of purely mental derangements and underrates and even omits his accompanying physical symptoms. The somapsychoses simulate or mimic physical and organic troubles. Thus psychosomatic forms simulate tabes, paralysis agitans, hemiplegia, paraplegia or epilepsy; while many neurasthenic, hypochondriacal and their allied states simulate visceral disturbances,―tumor or cancer of the stomach, intestinal obstruction, glandular derangements, cardiac, laryngeal, pneumonic, hepatic, splanchnic, ovarian, tubal, uterine and various other bodily afflictions. The psychoneuroses on the other hand resemble or simulate all forms of mental diseases, beginning with melancholia and mania and ending with general paresis and dementia præcox. All forms of mental obsessions are specially characteristic of psychoneurosis. All psychopathic affections, both somopsychosis and psychoneurosis are at bottom disturbances of associative activity, ideational and emotional. They are essentially abnormal forms of mental association and dissociation.
VII The etiology of functional psychosis in its double manifestation of somopsychosis and psychoneurosis is not so evident. There are some psychopathologists who refer functional psychosis to mental repression of the sex instinct. This etiology is strained and not in accordance with an unbiased study of clinical facts. In my clinical investigations, covering a number of years, I invariably find that it is the fear instinct awakened to abnormal activity that gives rise to all forms of functional psychosis in its two varieties of somopsychosis and psychoneurosis. We may say unhesitatingly that the causation of all psychopathic diseases can be referred to the fundamental instinct, not of sex or preservation of the species as some, seem to think, but to the fundamental instinct of self-preservation as manifested in the instinct of fear with its concomitant manifestation of the feeling of anxiety.9 I may say that this etiology is firmly established by my clinical studies in all the cases that have come under my observation and treatment. This fear instinct of self-preservation may be present subconsciously or consciously. In the somopsychoses the abnormal fear instinct is mainly subconscious, while in the psychoneuroses the fear instinct may rise to the surface of consciousness. Functional psychosis in its last analysis is a veiled form of the instinct of self-preservation, of the fear of death, of fear of loss of what is essential to life, of fear of some impending evil. The intense unconscious manifestations of egotism which so strongly permeates the life of psychopathic patients is but one manifestation of the instinct of self-preservation, of fear rooted in the fundamental impulse of self-preservation characteristic of all life.
VIII The general practitioner should have in mind the mental factor in the many forms of symptom-complexes under his care. He should further bear in mind that at least seventy-five per cent of the patients that come to him for treatment are psychopathic in character, psychosomatics or psychoneurotics in one form or another. The general practitioner should learn to diagnose the psychic origin of many a symptom-complex apparently physical in its manifestations. Not only will the patient benefit by a medical scientific treatment, but there will be less occasion for the many mystical, occult cults, Christian Science, New Thought, as well as prize-fighter treatments, absurd food cures, quasi-scientific and pseudo-hygienic doctors, mental healers who, like poisonous weeds, have overrun our country from ocean to ocean and threaten to undermine the health and to deteriorate the intelligence of the nation.
REFERENCES 1. Darwin, Ch.―The Expression of the
Emotions.
|