Home Boris Sidis Archives Table of Contents Next Chapter
|
PSYCHOPATHOLOGICAL
RESEARCHES Boris Sidis, M. A., Ph.D.,
M.D. © 1908
|
Mental Dissociation In Functional Motor Disturbances
By
GEORGE M. PARKER
CHAPTER I
HISTORY AND EXAMINATION
CASES of motor disturbances apparently due to no organic cause are becoming more frequently noted in psychopathological literature. While possessing their own individual features, all such cases present certain elements in common, to which we would direct the reader's attention.
Miss A., the patient, is twenty-five years of age. The family history contains certain determining factors. The paternal grandmother is described as having been a willful, unmanageable individual. The patient's father possesses many traits apparently derived from this genealogical branch. He is highly emotional, excessively sentimental, readily unbalanced, a very poor sleeper, an active dreamer, though not somnambulistic. Maternal side presents no point of interest. To neither side can presence of definite, transmitted disease be traced.
Personal history details an almost complete absence of ordinary somatic diseases of childhood and adolescence,―no diphtheria, no scarlatina, no rheumatism, no cholera, no trace of tuberculosis either pulmonary or articular, no anæmia, no trauma. Menstruation was established at the age of sixteen; it has been regular, though occasionally painful.
Further investigation, however, discloses the development of certain innate peculiarities, further accentuated by the action of environing conditions. Primarily, the resemblance to her father is marked.
As a child the patient was bright, but entirely lacking in persistency of purpose and action. The patient is described as irresponsible and eccentric. As possessor of a brighter, if less responsible, mind than the sister, her life has been that of constant favoritism, with the consequent wider divergence of these primary deviations. Succeeding years have exaggerated rather than ameliorated these peculiarities. Of especial interest is the undoubted existence of somnambulistic tendencies in childhood persisting up to adolescence. Her dream life has been active; content of dreams is distinctly unpleasant.
The accident, initiating the present illness, occurred two years ago. It was apparently a simple sprain, induced by foot turning, while walking a heavy country road in a light house slipper. Considerable pain attended the accident: There was the usual swelling, tenderness, etc., with no evidence of a fracture. Ordinary methods for reduction of swelling were employed followed by applications of a Gibney plaster. Although the foot apparently mended exceedingly well, the physician in attendance was greatly puzzled by the excessive general pain declared by the patient as accompanying the slightest movement. Frequent readjustment of the straps failed to remedy this condition. Patient finally attempted to walk after removing straps. She succeeded only in augmenting the symptoms. At this point she was advised, one month after the accident, to employ crutches. Since this time, she has continually used them. At the end of three months, patient's condition was unchanged. The swelling was slight, but the pain was excessive. The medical adviser again insisted upon patient's walking. A commiserating family and diminishing initiative defeated him. As the Gibney straps were sti1l maintained, walking with the leg suspended naturally produced a slight degree of stasis in the toes. Its increase was very gradual until six months later. During this interim, the patient had seen several surgeons in New York, both general and orthopædic. Their diagnoses were largely negative, but the questions directed to the patient made a deep impression on her. At this time the persistency of the pain, coincident with a marked increase of the œdema, led to her admission to the hospital. The œdema was not confined to the foot, but invaded the leg to the region of knee. Shortly after admission to hospital, a distinct bluish coloration appeared at the toes, extending upward and over the area of the œdema. Œdema and coloration controllable only by elevation of foot. Foot gradually assumed position of equino-valgus. Repeated examinations of foot by the surgeons could disclose no articular lesions. A plaster cast was applied to prevent further deformity. The patient was seen by a consulting neurologist, and the opinion of hysteria was advanced. From this time, galvanization and massage were intermittently applied. Contrary to advice of surgeons, patient refused to leave until one year after admission. Her condition, when discharged, was unimproved.
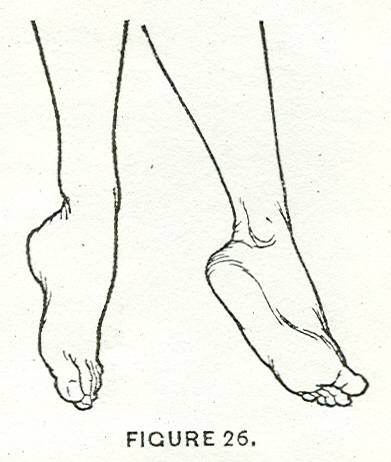
Previous to discharge, a skiagraph of the joint revealed an apparently normal condition, both of the bone and membrane. It was my good fortune to see this case directly after patient's discharge from hospital. The joint in question presented a rather startling appearance, both in its relative and real position. It rested upon a level higher than the patient's head; the only level in which it could be maintained without the appearance of œdema. The position assumed was that of marked equino-valgus.
There was no swelling about the joint. Bony prominences were distinct. Examination produced a characteristic display. At whatever point pressure might be exerted, an exceedingly vigorous reaction was manifested. Especially was this true over the malleoli, os calcis, along the entire extent of the tibia,―in short, wherever bony structures were superficial and apparent to the touch. The focus of greatest intensity could readily be varied by diversion of attention. A similar variability of reaction was noted towards stimuli of touch, pain, and temperature. Over the mesial surfaces of the foot, the reaction was rather delayed than diminished. Hypoæsthesia was demonstrable in kinæsthetic sensibility. Passive motion was impossible, every attempt to move foot apparently producing great pain. The joint furthermore was exceedingly rigid, antagonistic muscle groups being decided agents in this result. Active motion exhibited only a feeble movement of the toes. This slight movement was accompanied by violent protestations of inability, with equally violent contractions of opposing muscle groups.
After a brief, but painful struggle, the equilibrium between flexion and extension was disturbed, with resultant production of slight movement. There was considerable atrophy of the posterior parts of the leg.
No suspicion of tubercular disease could be entertained after examination of the joint, although by direct questioning, grounds for almost any diagnosis could be obtained. Demonstration of œdema was readily afforded by lowering the level of the foot. It rapidly appeared, beginning in the toes, and extended upward to the knee, a dark bluish coloration immediately following, its limits being coterminous with those of the œdema. This coloration was general; it was not preceded by sudden pallor. Slight drop in local surface temperature was evident. Considerable pain accompanied the appearance of œdema and coloration: There was no bilateral display of these symptoms at this time, no tenderness along the course of nerves. There was gradual disappearance of all symptoms upon re-elevation of foot.
![]()